Table of Contents >> Show >> Hide
- What Is ORIF Surgery, Exactly?
- When Is ORIF Surgery Needed?
- How Doctors Decide Whether ORIF Is the Best Option
- How ORIF Surgery Is Done
- What Recovery After ORIF Looks Like
- Risks and Possible Complications of ORIF Surgery
- Warning Signs After ORIF That Should Not Be Ignored
- Questions to Ask Before Having ORIF Surgery
- The Real-World Experience of ORIF Recovery
- Final Thoughts
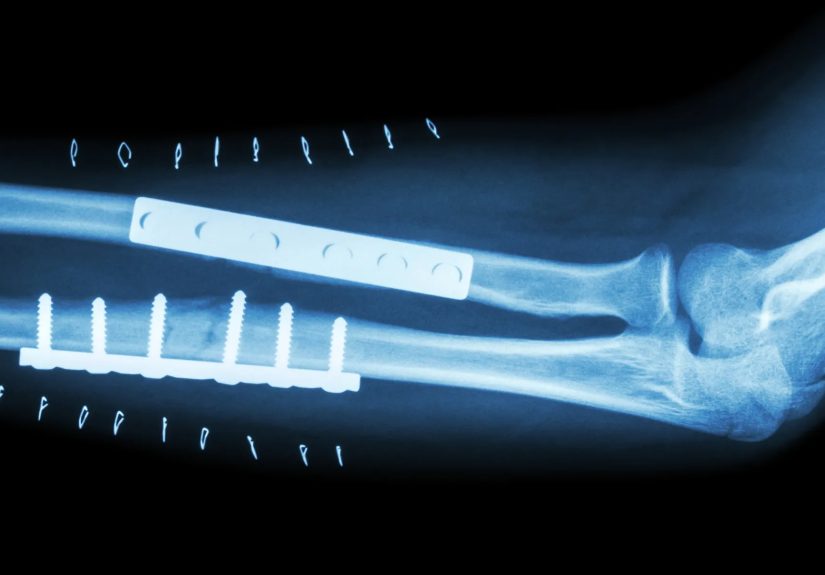
Broken bones are common. Broken bones that behave like rebellious furniture parts scattered across the floor are a different story. That is where ORIF surgery comes in. Short for open reduction and internal fixation, ORIF is a surgical method used to put fractured bones back where they belong and hold them there with hardware such as plates, screws, rods, pins, or wires while healing happens.
For many fractures, a cast, brace, or splint does the job just fine. But when a break is badly displaced, unstable, involves a joint, breaks through the skin, or shatters into several pieces, a simple cast may be about as helpful as taping together a cracked coffee mug and hoping for the best. In those cases, ORIF can help restore alignment, improve function, and reduce the risk of the bone healing in the wrong position.
This guide explains when ORIF surgery is needed, how ORIF is done, what recovery looks like, what risks come with the procedure, and what patients often experience once the operating room lights go off and real life begins.
What Is ORIF Surgery, Exactly?
ORIF has two parts, and the name is surprisingly literal.
Open reduction
The surgeon makes an incision to reach the broken bone and move the fragments back into their normal position. “Reduction” means restoring alignment. “Open” means it is done surgically through an incision rather than by manipulating the bone from the outside.
Internal fixation
Once the fracture is lined up, the surgeon secures it with internal hardware. Depending on the location and pattern of the fracture, that hardware may include:
- Plates and screws
- Intramedullary nails or rods
- Pins or wires
- Specialized fixation devices designed for certain bones or joints
The goal is simple: keep the bone stable enough to heal correctly. Think of the hardware as an internal cast with better engineering and worse dinner-party appeal.
When Is ORIF Surgery Needed?
Not every fracture needs surgery. In fact, many do not. Doctors usually prefer the least invasive treatment that can still give the bone a strong chance to heal in good alignment. But ORIF is often recommended when a fracture is unlikely to heal properly with conservative treatment alone.
Common reasons a patient may need ORIF
- Displaced fracture: the bone pieces are out of alignment
- Open fracture: the broken bone has punctured the skin
- Comminuted fracture: the bone has broken into several pieces
- Unstable fracture: the break is likely to shift even if placed in a cast
- Joint involvement: the fracture extends into a joint and needs precise restoration
- Associated dislocation: the injury includes both a fracture and a joint out of place
- Failed closed reduction: the bone cannot be aligned or kept aligned without surgery
- Functional demands: the patient needs reliable restoration of movement and strength
Doctors also weigh factors such as age, bone quality, swelling, blood supply, nerve or vessel injury, smoking status, diabetes, osteoporosis, and how active the patient is likely to be after recovery.
Fractures commonly treated with ORIF
ORIF is often used for fractures of the:
- Ankle
- Wrist, especially distal radius fractures
- Elbow
- Upper arm or humerus
- Clavicle
- Hip and femur
- Tibia and fibula
- Foot, including some metatarsal and Lisfranc injuries
- Kneecap in selected severe cases
In other words, if a major bone or joint takes a bad hit and the pieces are no longer playing nicely together, ORIF may enter the chat.
How Doctors Decide Whether ORIF Is the Best Option
Orthopedic surgeons do not choose ORIF based on one X-ray alone. The decision usually comes from a full evaluation that includes:
- A physical exam
- X-rays to define the fracture
- Sometimes a CT scan for complex or joint-related fractures
- Occasionally an MRI when soft-tissue injuries also matter
- An assessment of skin condition, swelling, and circulation
- A review of medications, allergies, and medical conditions
Sometimes surgery happens urgently. Other times, the team waits a short period for swelling to improve before operating. That pause can feel frustrating to patients, but it is often done to reduce complications and give the soft tissues a better chance.
How ORIF Surgery Is Done
If you have ever wondered what actually happens during open reduction and internal fixation, here is the standard playbook.
1. Preoperative preparation
Before surgery, the patient is evaluated and imaged. The care team reviews medications, especially blood thinners, and gives instructions about fasting. Some ORIF procedures are scheduled. Others happen the same day or shortly after injury, especially if the fracture is severe or unstable.
2. Anesthesia
ORIF is usually done under general anesthesia or regional anesthesia with sedation. The choice depends on the bone involved, the patient’s health, and the surgical plan.
3. Incision and exposure
The surgeon cleans the area and makes an incision through the skin and soft tissue to reach the fracture. The exact size and location vary by bone and fracture pattern. Some approaches are more minimally invasive than older techniques, but ORIF still involves direct surgical access.
4. Reduction
The broken pieces are moved back into alignment. This is the heart of the operation. If the bone heals crooked, the patient may be left with pain, weakness, stiffness, or altered joint mechanics. Good reduction matters because function later depends on what happens now.
5. Internal fixation
Once alignment looks right, the surgeon secures the fracture with hardware. The type depends on the injury:
- Plates and screws are common in ankle, wrist, clavicle, and some arm fractures
- Rods or nails are common in long bones such as the femur and tibia
- Pins or wires may be used in smaller bones or specific fracture patterns
In some cases, the surgeon also repairs nearby ligaments, tendons, cartilage, or other damaged structures. Then the incision is closed, dressed, and the limb may be placed in a splint, boot, brace, or cast.
6. Postoperative imaging and recovery room care
After surgery, patients are monitored while they wake up from anesthesia. Follow-up imaging may be used to confirm the hardware position and fracture alignment. Pain control starts immediately, and weight-bearing or activity restrictions are explained before discharge.
What Recovery After ORIF Looks Like
ORIF recovery depends on the bone, the severity of the fracture, the condition of the soft tissues, and the patient’s overall health. Recovery is not one-size-fits-all. A hand fracture and a femur fracture live in very different neighborhoods.
The first few days
Pain, swelling, bruising, and fatigue are common after surgery. The surgical site may feel tight, sore, and annoyingly dramatic. Patients are usually told to elevate the limb, protect the incision, and follow instructions about showering, dressing changes, and medication.
Early follow-up
Follow-up visits often happen within the first one to three weeks, depending on the injury. Stitches or staples may be removed, X-rays may be repeated, and the surgeon checks that the incision looks healthy and the hardware is doing its job quietly and without rebellion.
Weight-bearing and motion
This is where patients often get humbled. Many people feel better before the bone is actually ready. Depending on the fracture, the surgeon may restrict weight-bearing for weeks. In foot and ankle injuries, this can be especially strict. In some upper-extremity fractures, early motion is encouraged to reduce stiffness. Either way, the schedule should come from the surgeon, not from optimism.
Physical therapy
Some patients need formal physical or occupational therapy. Rehab may focus on range of motion, swelling control, strength, balance, gait training, grip, or fine motor use. The goal is not just bone healing but returning the limb to useful life.
How long does healing take?
Bone healing timelines vary widely. Some smaller fractures may allow return to work or sports in roughly two to three months, while larger injuries can take much longer. For example, recovery after femur fracture repair may stretch into several months. The larger and more complex the fracture, the more patience it tends to demand.
Will the hardware stay in forever?
Usually, yes. Many plates, screws, and rods are designed to stay in the body long term. Hardware removal is sometimes done if the implant causes pain, irritation, mechanical problems, or other complications, but routine removal is not always necessary.
Risks and Possible Complications of ORIF Surgery
Most ORIF procedures go well, but this is still surgery, which means there are real risks. These may include:
- Infection at the incision or deeper around the hardware
- Bleeding
- Nerve or blood vessel injury
- Blood clots
- Skin or soft-tissue complications
- Hardware irritation, loosening, breakage, or prominence
- Stiffness or reduced range of motion
- Malunion, nonunion, or delayed healing
- Need for repeat surgery
- Complications related to anesthesia
Some factors raise complication risk, including smoking, diabetes, poor bone quality, severe soft-tissue injury, and certain complex fracture patterns. Patients with implants should also know that hardware, like any device, can occasionally move, fail, or require later revision.
Warning Signs After ORIF That Should Not Be Ignored
Call the surgeon or seek urgent care if any of the following show up after ORIF:
- Fever
- Increasing redness, warmth, or drainage from the incision
- Severe pain that is worsening rather than improving
- Numbness, tingling, or loss of feeling
- Blue, purple, or cold fingers or toes
- Chest pain or shortness of breath
- Swelling that suddenly becomes much worse
Most healing is boring, which is good. Sudden drama is usually not the kind of plot twist you want after surgery.
Questions to Ask Before Having ORIF Surgery
Patients do better when they understand the plan. Useful questions include:
- Why is ORIF better than a cast or brace for this fracture?
- What type of hardware will be used?
- Will I be non-weight-bearing, and for how long?
- When can I drive, work, or return to sports?
- Will I need physical therapy?
- What warning signs mean I should call right away?
- How likely is it that the hardware will need to be removed later?
- What factors in my health make healing easier or harder?
The Real-World Experience of ORIF Recovery
Here is the part many medical articles rush past: what ORIF surgery recovery often feels like in ordinary life. Not the polished brochure version. The real version, where the cast is heavy, the shower is confusing, the stairs look rude, and your body suddenly turns into a project manager with terrible communication skills.
For many patients, the first surprise is that the fracture and the surgery are two different sources of discomfort. There is pain from the injury itself, and then there is soreness, swelling, and stiffness from the operation. Even when the surgery goes well, the area can feel tight, hot, puffy, and strange. A lot of people expect to feel dramatically better once the bone is “fixed,” but early recovery is usually more like controlled chaos than instant relief.
Swelling is one of the biggest recurring complaints. Patients often notice that the limb feels more swollen at the end of the day, after time upright, or after trying to do too much too soon. Elevation helps. Ice may help if the surgeon allows it. But patience is the real long game. Swelling can linger longer than people expect, especially in the foot, ankle, hand, and wrist.
Then there is the mental part. Patients commonly describe the odd frustration of feeling motivated while being medically benched. You may feel alert, restless, and ready to “get back to normal,” while your surgeon is telling you not to put weight on the leg, not to lift with the arm, or not to rush the range-of-motion exercises. That mismatch can be emotionally tiring. Recovery is not just physical; it is an exercise in restraint.
Daily routines also become strangely complicated. Showering turns into a weatherproofing project. Getting dressed may require strategy. Sleeping can be awkward because the limb has to be elevated or protected. Even simple tasks such as opening jars, carrying groceries, standing at the sink, or stepping off a curb can feel like advanced-level biomechanics. Patients with lower-extremity ORIF often discover that crutches, walkers, scooters, or boots are less glamorous than television has suggested. Patients with upper-extremity ORIF discover how often they use two hands without ever noticing it before.
Another common experience is stiffness. This can be especially frustrating because patients sometimes assume stiffness means something is wrong. Often, it is a normal part of the process. A repaired wrist may feel weak and wooden for a while. An ankle may feel rusty. Fingers may feel puffy and less coordinated. Movement usually improves gradually with time, guided exercises, and therapy when prescribed. That said, the key word is gradually. Recovery prefers inches over fireworks.
Follow-up visits also shape the emotional rhythm of healing. Patients often live from X-ray to X-ray, waiting for the words “it looks like it’s healing well.” Those visits matter because progress is not judged by vibes alone. A person may feel better and still not be ready for full activity. Or they may feel stiff and worried while the bone is healing exactly as expected. Imaging helps separate fear from fact.
Perhaps the most universal ORIF experience is this: recovery is rarely a straight line. One day feels encouraging, the next feels slower, and then things improve again. That is normal. The most successful patients are usually not the ones who heal fastest. They are the ones who respect the plan, protect the repair, keep follow-up appointments, and let biology work at its maddeningly nonnegotiable pace.
Final Thoughts
ORIF surgery is one of the most important tools in modern fracture care. When a bone is badly displaced, unstable, or too complex for a cast alone, open reduction and internal fixation can restore alignment, protect joint function, and improve the chances of a stronger recovery. The procedure is highly structured: realign the bone, stabilize it internally, protect it while it heals, and then rebuild movement and strength over time.
The catch, of course, is that good surgery is only part of the story. Recovery still requires wound care, follow-up, patience, and real respect for restrictions. Bones are impressive, but they do not enjoy being rushed. When patients understand why ORIF is needed and what the healing process actually involves, the whole experience becomes less intimidating and a lot easier to navigate.






