Table of Contents >> Show >> Hide
- Introduction: When Hospital Computers Became Emergency Patients
- What Happened During the WannaCry Cyber Attack?
- How UK Hospitals Were Crippled
- How the Attack Spread Globally
- The Technical Cause: A Known Vulnerability Left Unfixed
- Who Was Behind WannaCry?
- Why Hospitals Are Prime Ransomware Targets
- Lessons for Healthcare Cybersecurity
- Why This Attack Still Matters Today
- Real-World Experience: What the WannaCry Crisis Teaches Teams on the Ground
- Conclusion: The Real Cure Is Resilience
Note: This article treats the headline as referring primarily to the 2017 WannaCry ransomware outbreak, one of the most disruptive cyber attacks ever to hit the United Kingdom’s National Health Service and one of the clearest examples of how a hospital cyberattack can become a worldwide emergency almost overnight.
Introduction: When Hospital Computers Became Emergency Patients
Hospitals are supposed to treat emergencies, not become one. But during the WannaCry ransomware attack, the UK’s National Health Service found itself in exactly that uncomfortable position: computers locked, appointments canceled, emergency departments strained, and staff suddenly forced back into the land of paper notes, phone calls, and the kind of controlled chaos nobody misses from the pre-digital era.
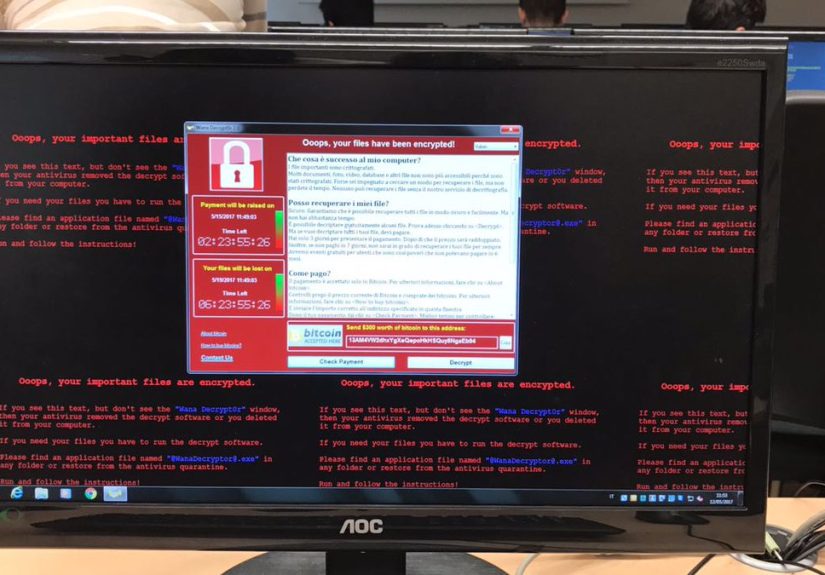
The massive cyber attack that crippled UK hospitals did not stop at Britain’s borders. It spread globally, striking hundreds of thousands of computers across countries, industries, and public services. The malware, known as WannaCry or WannaCrypt, behaved like ransomware with a jet engine strapped to it. It encrypted files, demanded payment in Bitcoin, and moved rapidly across vulnerable Microsoft Windows systems by exploiting an unpatched security flaw.
For healthcare leaders, IT teams, cybersecurity professionals, and ordinary patients, the incident became a brutal wake-up call. It showed that cybersecurity is not just an IT department problem. In a hospital, a locked computer can delay a blood test, block access to patient records, disrupt radiology, cancel surgery, or force ambulances to drive elsewhere. In other words, cyber resilience is patient safety wearing a hoodie.
What Happened During the WannaCry Cyber Attack?
On May 12, 2017, WannaCry began spreading rapidly around the world. Unlike many ransomware attacks that rely mainly on phishing emails, this malware used a worm-like capability to move automatically between vulnerable machines. Once inside a network, it searched for other exposed systems and infected them too. That made it especially dangerous for large organizations with old machines, flat networks, and delayed patching.
The ransomware targeted Microsoft Windows systems that had not installed a critical security update. Microsoft had released a fix before the attack, but many organizations had not applied it in time. That delay turned a known vulnerability into a global crisis. The lesson was painfully simple: a patch sitting unapplied is like a locked fire extinguisher during a kitchen fire.
In the UK, the NHS was not believed to be the specific target, but it became one of the most visible victims. Hospitals and general medical practices were disrupted, staff lost access to important systems, and some emergency care had to be redirected. The attack exposed how dependent modern healthcare had become on digital records, scheduling systems, diagnostic tools, email, and networked devices.
How UK Hospitals Were Crippled
The impact on NHS England was severe. Dozens of trusts and hundreds of primary care organizations were affected. Some organizations were directly infected, while others shut down systems as a precaution. That distinction matters technically, but for patients waiting for care, the result felt very similar: delays, cancellations, and confusion.
Thousands of appointments and operations were canceled. Some accident and emergency departments could not treat certain patients, forcing ambulances and patients to travel farther. Hospitals had to fall back on manual processes, including paper records and telephone-based coordination. It was a reminder that when digital systems fail, the backup plan cannot be “everyone panic elegantly.”
Healthcare staff responded with grit. IT teams worked through the weekend. Clinicians improvised. Administrators coordinated emergency communications. But the incident revealed major weaknesses: outdated software, inconsistent patching, unclear response leadership, and insufficient rehearsal for a national cyber incident.
Why the NHS Was So Vulnerable
WannaCry did not succeed because it was magical. It succeeded because it found familiar weaknesses at scale. Many healthcare systems rely on legacy technology because medical software can be expensive, hard to replace, and difficult to patch without risking downtime. Hospitals operate 24/7, so taking systems offline for maintenance can feel like changing the tires on an ambulance while it is moving.
But attackers do not care whether patching is inconvenient. They care whether a door is open. In the WannaCry case, unpatched systems, network exposure, and inconsistent local readiness created the conditions for widespread disruption. The attack proved that cybersecurity debt works like medical debt: ignore it long enough, and eventually the bill arrives with interest.
How the Attack Spread Globally
WannaCry was global because the vulnerability it exploited was global. Companies, government agencies, transportation providers, manufacturers, telecom firms, and healthcare organizations all used affected Windows systems. The malware did not need a passport. It moved through networks wherever vulnerable machines were reachable.
Victims were reported across many countries and sectors. Well-known organizations outside the NHS, including major manufacturers and shipping-related businesses, experienced disruption or took systems offline to contain risk. The outbreak became a symbol of how interconnected the digital world had become. One leaked exploit, one missed patch, and one fast-moving worm were enough to create worldwide operational pain.
The cyber attack also showed that ransomware had evolved. It was no longer just a nuisance that locked one unlucky employee’s files. It could interrupt national healthcare services, delay transportation, disrupt factories, and force executives into emergency meetings where the phrase “Do we have clean backups?” suddenly became the most important sentence in the room.
The Technical Cause: A Known Vulnerability Left Unfixed
At the center of WannaCry was a Windows vulnerability associated with Server Message Block, commonly called SMB. SMB helps computers share files, printers, and other resources across a network. That usefulness also made it dangerous when exposed or left unpatched.
The exploit used by WannaCry became widely known as EternalBlue. Microsoft had released a security update before the outbreak, but vulnerable systems remained. Once WannaCry infected one machine, it could scan for others and spread automatically. That worm behavior turned a ransomware incident into a digital wildfire.
The fix was not mysterious. Patch vulnerable systems. Reduce unnecessary exposure of SMB services. Segment networks so one compromised device cannot easily infect everything else. Maintain tested backups. Monitor for abnormal behavior. Practice response plans before the sirens go off. None of that sounds glamorous, but glamour has a poor track record in cybersecurity. Boring controls save the day.
Who Was Behind WannaCry?
U.S. and allied officials later attributed the WannaCry attack to North Korea-linked actors, commonly associated with the Lazarus Group. The U.S. Department of Justice later described allegations involving North Korean state-backed cyber activity, including the creation of malware used in the WannaCry 2.0 attack. Treasury officials also linked Lazarus Group to the destructive ransomware outbreak.
Attribution in cyber incidents can be complex. Attackers route traffic through other countries, reuse code, steal tools, and plant false clues. Still, the official public position from the United States and several partners was clear: WannaCry was not simply the work of a basement prankster with too much caffeine. It was treated as a serious state-linked cyber operation with global consequences.
Why Hospitals Are Prime Ransomware Targets
Hospitals are attractive to ransomware gangs for several reasons. They store valuable personal and medical data. They rely on uptime. They use specialized equipment and software that may be difficult to update. They also face intense pressure to restore services quickly because patient care cannot simply be paused like a streaming subscription.
That pressure creates leverage. If a factory goes down, production stops. If a hospital goes down, people may wait longer for urgent care. Cybercriminals know this, which is why healthcare ransomware remains a major threat. The most dangerous part is not always stolen data; sometimes it is operational paralysis.
WannaCry made this visible to the public. Suddenly, ransomware was not an abstract cybersecurity term. It was a reason an appointment might be canceled, an ambulance diverted, or a clinician unable to access a digital system at the exact moment it was needed.
Lessons for Healthcare Cybersecurity
1. Patch Management Is Patient Safety
The biggest lesson is that patch management must be treated as a clinical risk issue, not merely a technical chore. When a vulnerability can interrupt care, applying security updates becomes part of protecting patients. Hospitals need asset inventories, patch timelines, exception tracking, and executive oversight.
2. Network Segmentation Limits the Blast Radius
If every device can freely talk to every other device, ransomware gets a free tour of the building. Network segmentation helps contain malware by separating critical systems, backups, medical devices, administrative machines, and guest networks. Think of it as hospital fire doors for data.
3. Backups Must Be Clean, Offline, and Tested
Backups are not useful if ransomware can encrypt them too. Healthcare organizations need offline or immutable backups, regular restore testing, and clear recovery priorities. A backup strategy that has never been tested is more of a hope than a plan.
4. Incident Response Plans Need Rehearsal
During WannaCry, communication challenges appeared quickly because email and other systems were affected. Hospitals must rehearse cyber incidents the way they rehearse clinical emergencies. Who leads? Who calls regulators? How do departments communicate if email is down? Which systems come back first? These answers should not be invented at 2:00 a.m. while a ransom note is blinking on the screen.
5. Cybersecurity Requires Board-Level Attention
Cybersecurity is often discussed in technical language, but the risk is operational, financial, legal, and clinical. Boards and executives should understand ransomware exposure, funding needs, recovery readiness, and third-party risks. A hospital cannot outsource accountability just because it outsourced a system.
Why This Attack Still Matters Today
WannaCry is no longer breaking news, but its lessons are still fresh. Modern ransomware groups are faster, more organized, and often more ruthless. Many now steal data before encrypting systems, creating double extortion: pay to restore operations and pay again to prevent leaks. Healthcare organizations also rely more heavily on cloud services, connected medical devices, remote access tools, and third-party vendors.
The same basic weaknesses still matter: unpatched systems, weak access controls, poor visibility, exposed services, inadequate backups, and slow response. Technology changes, but ransomware criminals continue to love the classics. They do not need to defeat a perfect security program; they only need to find the one forgotten server everyone assumed someone else was maintaining.
Real-World Experience: What the WannaCry Crisis Teaches Teams on the Ground
The most useful experience from the WannaCry hospital cyberattack is not just technical. It is human. When computers lock up in a healthcare setting, the first shock is emotional. Staff members are trained for medical emergencies, but a digital emergency feels different. Screens freeze. Printers stop. Phones become overloaded. Nobody knows whether the problem is local, regional, or national. The first hour is often filled with uncertainty, and uncertainty is where bad decisions breed like rabbits in a vegetable garden.
One practical lesson is that hospitals need downtime playbooks that staff can actually use. A beautiful 80-page incident response document is not helpful if nobody can find it during a crisis or if it lives on the very network that just got encrypted. Departments need printed quick-reference guides, updated contact lists, and clear instructions for switching to manual workflows. The boring clipboard suddenly becomes a heroic object.
Another experience-based lesson is that communication must be redundant. During a ransomware outbreak, email may not work. Shared drives may be inaccessible. Internal messaging platforms may be offline. Teams need backup communication channels, such as emergency phone trees, secure messaging alternatives, radio systems, or predefined command centers. The message “turn off your computer” sounds simple until you realize half the staff did not receive it.
Clinical prioritization is also critical. Not every system can be restored first. A hospital must know which services are most essential to life and safety: emergency departments, intensive care, imaging, pathology, pharmacy, operating rooms, and patient records. Recovery should follow a triage model. Cyber incident response in healthcare is not just about restoring technology; it is about restoring care in the right order.
IT teams also learn that asset visibility is priceless. You cannot patch what you cannot see. You cannot isolate what you do not know exists. Hospitals often contain a messy mix of desktops, servers, lab systems, imaging equipment, vendor-managed devices, and legacy software that nobody wants to touch because it still “works.” WannaCry proved that “still works” is not the same as “still safe.”
Training matters too, but it must be realistic. Staff do not need to become cybersecurity engineers. They need to know how to report suspicious behavior, what to do when a ransom message appears, whom to call, and how to continue safe care during downtime. Good training turns panic into procedure.
Finally, the biggest experience from WannaCry is that recovery is a team sport. Cybersecurity teams, clinicians, administrators, vendors, executives, regulators, and communications staff all have roles. The organizations that respond best are not the ones that never face trouble. They are the ones that practice, communicate clearly, invest before disaster, and treat cybersecurity as part of the hospital’s duty of care.
Conclusion: The Real Cure Is Resilience
The massive cyber attack that crippled UK hospitals and spread globally remains one of the clearest warnings in modern cybersecurity. WannaCry proved that ransomware can jump from a technical vulnerability to a public health disruption in a matter of hours. It showed how old software, delayed patching, weak segmentation, and untested response plans can turn ordinary systems into points of failure.
But the story is not only about failure. It is also about resilience. NHS staff improvised under pressure. Security researchers helped slow the outbreak. Governments and technology companies learned hard lessons. Healthcare leaders around the world saw, in painfully practical terms, that cyber defense is not optional infrastructure. It is as essential as electricity, oxygen, and clean water.
The next hospital cyberattack may use different malware, a different exploit, or a different extortion model. But the defense will still depend on the fundamentals: patch early, segment networks, protect backups, train staff, rehearse response plans, and make cybersecurity a leadership priority. In healthcare, resilience is not just about keeping computers running. It is about keeping patients safe when the computers do not.






