Table of Contents >> Show >> Hide
- Quick Navigation
- What Exactly Is a Spiral Fracture (and Why Does It Look Like That)?
- Tibia vs Fibula: The Lower-Leg Duo (One Works Hard, One Multitasks)
- Symptoms, Diagnosis, and Red Flags (a.k.a. “Should I Google This or Go Now?”)
- Treatment Options: Cast, Boot, or Surgery (Choose Your Adventure)
- Spiral Fracture Healing Time: Tibia and Fibula Timeline (Realistic Milestones)
- What Changes Healing Time (and How to Stack the Odds in Your Favor)
- When Can You Walk Again? Weight-Bearing After a Tibia/Fibula Spiral Fracture
- Rehab & Physical Therapy: Getting Your Knee and Ankle Back Online
- Complications to Watch For (Because Google Won’t Mention the Boring Wins)
- FAQs: Spiral Fracture Healing Time, Tibia, and Fibula
- Bonus: Real-World Recovery Experiences After a Spiral Fracture (What People Commonly Report)
- Conclusion
A spiral fracture is the orthopedic version of a “plot twist”literally. Instead of a clean snap, the bone breaks with a corkscrew pattern after a twisting force. It’s dramatic, it’s painful, and it tends to show up in the lower leg where life loves to test your balance, your footwear choices, and your patience.
This guide focuses on spiral fractures involving the tibia (your main weight-bearing shinbone) and the fibula (its slimmer sidekick). We’ll cover realistic healing times, treatment paths (cast vs surgery), weight-bearing milestones, rehab, complications to watch for, and what recovery typically feels like day to day.
Medical note: This article is for education, not a diagnosis. If you think you have a fractureor you have severe pain, numbness, an open wound, or your foot looks pale/coldseek urgent medical care.
What Exactly Is a Spiral Fracture (and Why Does It Look Like That)?
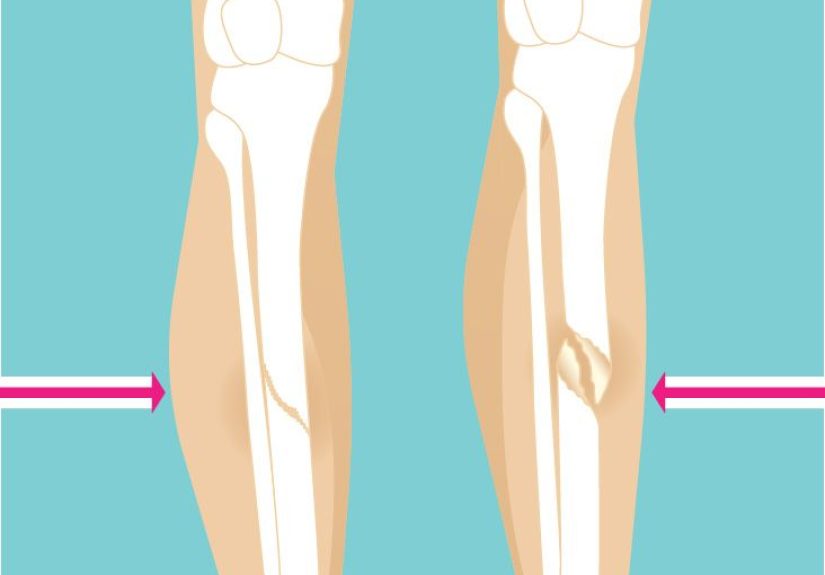
A spiral fracture is a complete break that wraps around the bone’s axisthink “candy cane stripe,” but way less festive. It typically happens when a twisting force travels through a bone faster than the bone can tolerate. The result is a fracture line that spirals along the shaft, especially in long bones like the tibia.
Common ways people earn this injury (unfortunately)
- Sports twisting injuries: A planted foot plus a rotating body (basketball, soccer, football).
- Skiing mishaps: Your ski catches; your leg disagrees.
- Falls: Especially if you twist while going down.
- Car or motorcycle crashes: High-energy trauma can produce complex spiral patterns.
Spiral fractures can be non-displaced (bones still aligned) or displaced (misaligned). That one detailalignmentoften decides whether you’re in a cast watching reality TV or meeting an orthopedic surgeon and a collection of metal hardware.
Tibia vs Fibula: The Lower-Leg Duo (One Works Hard, One Multitasks)
The tibia: your body’s main “load-bearing column”
The tibia carries most of your weight. When it fractures, walking is usually not just “uncomfortable” it’s “absolutely not.” Tibial shaft fractures are common in major trauma and sports injuries, and they can require longer healing because the bone is doing heavy-duty work and has less forgiving blood supply in some areas.
The fibula: the sidekick with a real job
The fibula is thinner and not the primary weight-bearer, but it’s important for ankle stability, muscle attachment, and overall lower-leg structure. A spiral tibia fracture can happen with or without a fibula fracture. When both are involved, stability and treatment planning become more complex.
Translation: if the tibia is broken, the fibula can’t “pick up the slack.” It can, however, complicate alignment and affect how your ankle and knee feel during recovery.
Symptoms, Diagnosis, and Red Flags (a.k.a. “Should I Google This or Go Now?”)
Common symptoms of a spiral fracture in the lower leg
- Immediate pain (often severe) and tenderness along the shin or outer lower leg
- Swelling and bruising
- Deformity or the leg looking “not like it did five minutes ago”
- Inability to bear weight (especially with tibia involvement)
- Feeling or hearing a “pop” at the injury moment
How clinicians confirm it
Most spiral fractures are diagnosed with X-rays. If the fracture involves the joint surface (knee/ankle), or if the break pattern is complex, clinicians may order a CT and occasionally an MRI to assess ligaments or cartilage. A thorough exam also checks skin integrity, circulation, and nerve function.
Red flags that warrant urgent/emergency care
- Open fracture: bone breaks through skin (high infection risk)
- Numbness/tingling or inability to move toes
- Foot is cold/pale or pulses are weak
- Pain out of proportion or pain with stretching the toes/ankle (possible compartment syndrome)
Treatment Options: Cast, Boot, or Surgery (Choose Your Adventure)
First steps (what happens early)
Early care focuses on stabilizing the leg (splinting), controlling pain/swelling, and making sure circulation and nerves are intact. In higher-energy injuries, doctors also watch closely for swelling-related complications.
Non-surgical treatment: splint → cast/boot → gradual return
If the spiral fracture is stable and well-aligned (often non-displaced), treatment may be immobilization with a splint initially, followed by a cast or functional brace. In general, spiral fractures may require several weeks of immobilization, and the exact duration depends on bone, location, alignment, and your follow-up X-rays.
- Splints are often used early while swelling is high.
- Casts commonly stay on for weeks; follow-up imaging checks alignment and healing progress.
- Boots may be used for certain fibula/ankle-region patterns when appropriate.
Surgery: when alignment or stability needs “hardware help”
Surgery is more likely if the fracture is displaced, unstable, open, involves multiple fragments, or if both tibia and fibula injuries make alignment difficult. For tibial shaft fractures, a common surgical method is intramedullary nailing (a rod placed inside the tibia). Other cases may use plates and screws (ORIF), especially around joints.
The goal isn’t to turn you into a cyborg (though it can feel like it at airport security). The goal is stable alignment so the bone can knit together properly and you can move earlier and more safelyunder your surgeon’s plan.
Spiral Fracture Healing Time: Tibia and Fibula Timeline (Realistic Milestones)
The question everyone asks is also the question everyone hates hearing answered: “It depends.” But we can still give a realistic framework.
Typical healing time ranges (big-picture)
- Tibia (shinbone) fractures: many take roughly 4–6 months to heal completely, with more severe injuries taking longer.
- Immobilization windows: casts/boots are often measured in weeks (commonly 6–8 for certain patterns), but “bone fully healed” is measured in months.
- After tibial nailing: radiographic union is often discussed around the ~20-week range in some studies, but function and strength may continue improving long after.
- Kids heal faster: pediatric tibia/fibula fractures may use casting for weeks (often shorter than adult timelines, depending on age and pattern).
A practical spiral fracture recovery timeline (adult lower leg)
- Week 0–2: “Swelling, paperwork, and gravity is your enemy.”
Expect pain control, immobilization, elevation, and follow-up planning. If surgery was needed, this is the incision-care and “don’t do anything heroic” phase. - Week 2–6: Early healing + protected movement.
The body builds early repair tissue. Many patients remain non-weight-bearing or partial-weight-bearing depending on the fracture and treatment. Gentle range-of-motion work may begin if approved. - Week 6–12: Gradual progress (if X-rays cooperate).
Some rehab programs add more motion and strengthening around this window, and weight-bearing may increase stepwise. This is often when you start noticing which muscles went on vacation without telling you. - Month 3–6: “Back to normal-ish” for many, not all.
Many tibia fractures approach full bony healing in this range, but impact activities, long shifts standing, and sports may require additional time and clearance. - Beyond 6 months: finishing school for your leg.
Stamina, balance, and confidence can take longer than the bone itself. Some people feel great at 4–6 months; others take longerespecially after open fractures or joint involvement.
If you want a single takeaway: casts are counted in weeks, tibia healing is counted in months, and “feeling normal” can be a longer story.
What Changes Healing Time (and How to Stack the Odds in Your Favor)
Factors you can’t control (but your doctor will)
- Fracture severity and alignment: displaced, comminuted, or joint-involved fractures take longer.
- Open vs closed fracture: open fractures carry higher infection risk and may heal more slowly.
- Soft tissue damage: swelling and skin/muscle injury can delay rehab and surgery timing.
Factors you can control (yes, you matter here)
- Smoking/vaping nicotine: strongly associated with delayed bone healingthis is one of the biggest modifiable risks.
- Nutrition: adequate protein, calcium, and vitamin D support healing (ask your clinician if supplements are appropriate).
- Follow weight-bearing rules: “testing it” too early can cause loss of alignment or hardware problems.
- Physical therapy consistency: the best plan is the one you actually do.
- Chronic conditions: diabetes, vascular disease, and certain medications can affect healingcoordinate care early.
Bone healing is biology, but recovery is also behavior. The bone can be doing its job while you accidentally sabotage the process by turning “one quick step without crutches” into “one surprising trip back to the clinic.”
When Can You Walk Again? Weight-Bearing After a Tibia/Fibula Spiral Fracture
Weight-bearing is not a motivational quote; it’s a prescription. Some patients are allowed weight-bearing as tolerated relatively early after certain surgeries, while others must stay non-weight-bearing for weeks. It depends on stability, fracture type, fixation method, and your surgeon’s protocol.
Common phases you might hear
- NWB (non-weight-bearing): foot cannot touch down for support.
- TTWB (toe-touch weight-bearing): foot down for balance only, not load.
- PWB (partial): a percentage of body weight allowed (often progressed gradually).
- WBAT: as much as you can tolerate without breaking the rules.
- FWB: full weight-bearing, usually after evidence of healing and clinical stability.
The best advice is also the least exciting: follow the plan you were given. Your leg is not impressed by bravado. Your tibia, especially, prefers boring compliance.
Rehab & Physical Therapy: Getting Your Knee and Ankle Back Online
A lower-leg spiral fracture doesn’t just break bone; it disrupts movement patterns. After immobilization, stiffness and weakness are commonnot only in the injured area but sometimes above and below it (knee and ankle).
What rehab often targets
- Range of motion: especially ankle mobility and knee bending/straightening
- Strength: calf, shin muscles, quads, hamstrings, hip stabilizers
- Balance and gait training: re-learning to walk smoothly
- Swelling control: elevation, compression (if advised), and safe movement
Expect rehab to take months for many significant leg fractures. The bone may “heal,” but function continues improving with progressive loading and targeted exercises. Most clinicians care about both: X-ray progress and how you move in real life (stairs, uneven ground, longer walks, work demands).
Complications to Watch For (Because Google Won’t Mention the Boring Wins)
Most people heal well with proper treatment, but it helps to know what clinicians monitorso you can report symptoms early.
Potential complications
- Compartment syndrome: dangerous pressure buildupsevere escalating pain is a key warning sign.
- Infection: more common with open fractures or after surgery (watch for fever, drainage, worsening redness).
- Delayed union/nonunion: bone takes longer than expected to heal, or doesn’t heal without additional treatment.
- Malunion: bone heals in a less-than-ideal position, affecting gait and function.
- Blood clots (DVT): risk increases with immobilization; follow prevention guidance from your clinician.
- Stiffness and chronic swelling: common early; sometimes lingers for months.
Call your clinician if symptoms are worsening instead of gradually improvingespecially escalating pain, new numbness, fever, or sudden shortness of breath.
FAQs: Spiral Fracture Healing Time, Tibia, and Fibula
How long will I be in a cast or boot?
Immobilization commonly lasts several weeks (often in the 4–8 week ballpark for certain patterns), but it varies widely by bone, location, alignment, and whether surgery was done. Your follow-up X-rays matter.
Does a spiral fracture always need surgery?
No. If the fracture is stable and well-aligned, immobilization may be enough. Surgery becomes more likely with displacement, instability, open fractures, or complex tibia/fibula involvement.
Is the fibula “less serious” than the tibia?
The fibula is less weight-bearing, but fibula fractures can still be painful and functionally limitingespecially near the ankle. If the tibia is also fractured, the injury is generally more serious and recovery is usually longer.
When can I drive again?
Driving depends on which leg, whether you’re weight-bearing, pain control (no impairing meds), and reaction time. Many clinicians require you to be safely weight-bearing and able to perform emergency braking before clearing driving.
Bonus: Real-World Recovery Experiences After a Spiral Fracture (What People Commonly Report)
The internet is full of timelines that read like: “Week 1: cast. Week 2: vibes. Week 3: ran a marathon.” In real life, recovery from a spiral fractureespecially involving the tibiafeels more like a series of small wins stacked on top of occasional frustrations (and at least one dramatic moment involving a shower).
The first 7–10 days are often about logistics. People commonly describe learning the art of strategic elevation (pillows everywhere), keeping swelling down, and figuring out how to sleep when your leg feels like it’s auditioning to be a weather balloon. It’s also when you discover crutches have a personality: they’re helpful, but they will absolutely bruise your armpits if you use them wrong. Many patients say the hardest part early on isn’t painit’s losing independence for basic tasks like carrying a plate of food without growing a third arm.
Weeks 2–6 are frequently described as “quiet progress.” Pain often improves, but boredom increases. People report that friends check in less often once the initial drama fadesright around the time you would like an extra hand to move the laundry basket. Mentally, this phase can be tricky: you may feel better and get tempted to “just take a few steps.” A lot of patients say the most useful mindset shift is treating weight-bearing restrictions like a seatbelt: not optional, not negotiable, and absolutely there to prevent a worse problem.
Rehab and the return of movement can feel surprisingly emotional. Once you start physical therapy or approved exercises, people often describe the first ankle circles or knee bends as both exciting and humbling. The muscles around the injured leg may feel weaker than expected, and balance can be off even if the bone is doing fine. A common experience is “the fear step”the first time you put more weight through the leg and your brain hits the panic button before your bone has any actual complaint. Good therapists and gradual progression help retrain confidence.
Swelling and stiffness are also frequent characters in the story. Many people say swelling is worse at the end of the day, especially after returning to work or doing more walking. It can be discouraging because it feels like regression, but it’s often just the body adapting to increased activity. Elevation, compression when advised, and pacing (not doing all your errands on the same day like you’re making up for lost time) can make a big difference.
Returning to normal life is often non-linear. People commonly report they can do one big thinglike a longer walkthen feel “payback” the next day. Many say the best progress comes from consistency: small daily rehab work rather than occasional heroic workouts. And yes, people frequently mention a surprising milestone: the first time you walk without thinking about walking. It’s not always fast, but it’s a real momentlike your body finally stops running the “injury background app” at full volume.
If you’re in the middle of this recovery, the most common practical advice people share is simple: keep your follow-ups, do your rehab, eat like healing matters, and celebrate small milestones. Bone healing is a process; so is rebuilding your life around ittemporarily. (Also: buy the shower chair. Just trust me on that one.)
Conclusion
A spiral fracture of the tibia and/or fibula is a twisting injury with a very real recovery arc: immobilization and protection in the early weeks, gradual loading and rehab over months, and a longer “fine-tuning” phase where strength and confidence catch up to the X-ray.
Many tibia fractures take roughly 4–6 months to heal completely, while walking progression depends on stability, treatment type, and your clinician’s protocol. The smartest recovery plan is rarely the fastest-looking oneit’s the one that protects alignment, restores motion, rebuilds strength, and avoids setbacks.






