Table of Contents >> Show >> Hide
- What changed in the blood pressure guidelines?
- Blood pressure categories, translated into normal human language
- Why did experts lower the definition?
- What do the two numbers actually mean?
- Does a single high reading mean you have hypertension?
- When are lifestyle changes enough, and when do medications matter?
- The lifestyle moves that actually matter
- How to take your blood pressure at home without sabotaging the result
- When should you worry right away?
- Common mistakes people make when reading the guidelines
- Conclusion: how to read the new guidelines without overreacting
- Experiences People Commonly Have When Reading the New Blood Pressure Guidelines
- SEO Tags
If the phrase new blood pressure guidelines makes you want to sit down, uncross your legs, and stare suspiciously at a cuff, you are not alone. Blood pressure advice can feel strangely simple and wildly confusing at the same time. One moment you think you are “fine,” and the next a reading of 130/80 suddenly sounds like a plot twist. That is exactly why so many readers went looking for Harvard Health’s plain-English take on the updated numbers.
Here is the short version: the guidelines lowered the threshold for what counts as high blood pressure, and that matters because heart disease risk does not magically begin at 140/90. In other words, the newer approach asks people to pay attention earlier, not panic earlier. That is an important distinction. The goal is not to turn half the country into amateur cardiologists with kitchen-counter monitors and spreadsheets. The goal is to catch risk sooner, measure more accurately, and prevent heart attacks, strokes, kidney disease, and other complications before they crash the party.
This guide breaks down what the blood pressure numbers mean, why the threshold changed, when lifestyle changes may be enough, when medication enters the conversation, and how to avoid getting a fake high reading because your arm was floating in space like a confused flamingo. Let’s decode the numbers without the medical fog machine.
What changed in the blood pressure guidelines?
The biggest headline is this: high blood pressure, or hypertension, is now generally defined as a consistent reading of 130/80 mm Hg or higher. Older U.S. standards often used 140/90 as the main cutoff for many adults, and some older adults were given even higher thresholds. The updated approach reflects evidence showing that risk climbs before 140/90, especially for heart attack, stroke, heart failure, and kidney damage.
That does not mean one slightly high reading at the pharmacy kiosk means you have a lifelong label and a breakup text from your salt shaker. Diagnosis usually depends on repeated readings over time, often including home or out-of-office monitoring. The updated framework is less about slapping a scary word on people and more about creating earlier, smarter prevention.
Blood pressure categories, translated into normal human language
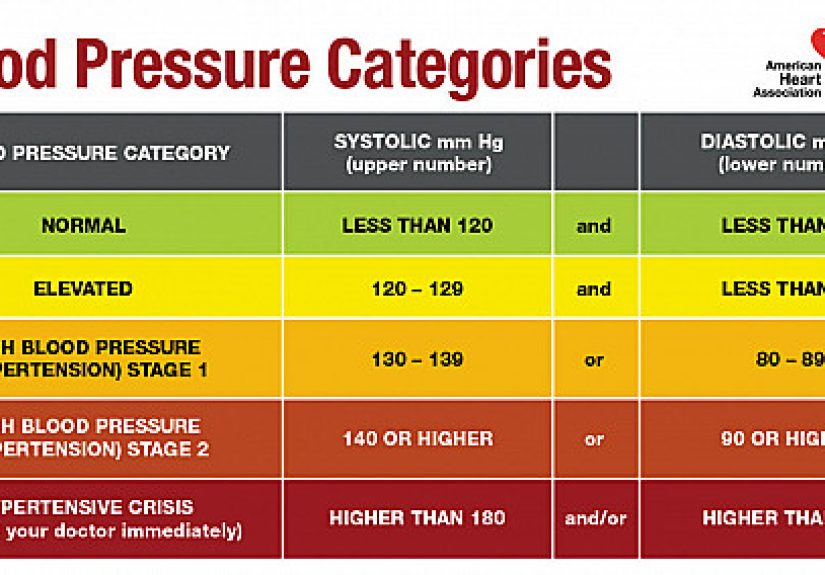
| Category | Systolic (top number) | Diastolic (bottom number) | What it means |
|---|---|---|---|
| Normal | Less than 120 | Less than 80 | Your numbers are in the healthy range. Keep doing the boring-but-brilliant basics. |
| Elevated | 120-129 | Less than 80 | Not hypertension yet, but it is a yellow light, not a confetti cannon. |
| Stage 1 hypertension | 130-139 | 80-89 | This is where the updated guidelines changed the conversation in a major way. |
| Stage 2 hypertension | 140 or higher | 90 or higher | This is a clearer signal that treatment, often including medication, may be needed. |
| Hypertensive crisis | 180 or higher | 120 or higher | This can be urgent or emergent, especially if symptoms are present. |
One detail people often miss: if your top and bottom numbers land in different categories, clinicians use the higher category. So a reading of 132/78 is treated as Stage 1 hypertension, not “basically normal because the bottom number behaved.” Blood pressure does not grade on a curve.
Why did experts lower the definition?
Because cardiovascular risk shows up earlier than many people assumed. Research behind the updated guidance, including the well-known SPRINT trial and related evidence reviews, helped push the idea that tighter control can protect the heart and brain more effectively for many adults. Harvard Health highlighted this shift because it changed not just the numbers, but the mindset: prevention should start before blood vessels have spent years getting roughed up.
This matters on a population level, too. Nearly half of U.S. adults meet criteria for hypertension, and many either do not know it or are not adequately controlled. High blood pressure is often called a “silent” condition for a reason. Most people do not feel it happening. There is no dramatic soundtrack, no villain monologue, and usually no obvious symptoms. That is why regular measurement matters so much.
What do the two numbers actually mean?
Systolic pressure, the top number, measures the pressure in your arteries when your heart beats. Diastolic pressure, the bottom number, measures the pressure between beats, when the heart relaxes. Both numbers matter. A high systolic value is common with aging because arteries can become stiffer over time, but a high diastolic value still counts and still deserves attention.
In practical terms, think of systolic as the pressure of the “push” and diastolic as the baseline tension in the system. If either number stays high over time, your arteries, heart, brain, kidneys, and eyes may pay the price.
Does a single high reading mean you have hypertension?
Usually, no. One isolated reading can be influenced by stress, caffeine, exercise, a full bladder, talking during the measurement, or the universal human experience of seeing a blood pressure machine and instantly becoming weird. Clinicians typically diagnose hypertension based on the average of multiple readings taken on separate occasions. U.S. screening guidance also supports confirming high office readings with measurements outside the clinic when possible.
That is where home blood pressure monitoring becomes useful. It can help confirm whether your pressure is truly high, reveal white coat hypertension where clinic readings run higher than usual, or uncover masked hypertension where office numbers look acceptable but home numbers are high. In other words, your blood pressure may have different manners at home than it does in public.
When are lifestyle changes enough, and when do medications matter?
This is where the guidelines become more nuanced than a simple chart. If you are in the elevated range, the main recommendation is usually lifestyle improvement: better diet, more activity, weight management if needed, better sleep, less alcohol, and less sodium. No mystery there. Your heart has been begging for that playlist for years.
If you are in Stage 1 hypertension, treatment depends on overall cardiovascular risk. For some adults, especially those with lower short-term risk, clinicians may recommend a dedicated period of lifestyle changes first, then reassess in a few months. But if you already have cardiovascular disease or your 10-year risk is high enough, medication may be recommended sooner rather than later.
If you are in Stage 2 hypertension, medication is much more likely to be part of the plan, often alongside lifestyle changes. And regardless of category, treatment goals often aim for blood pressure under 130/80 for many adults, depending on age, risk profile, and other medical conditions.
The important takeaway is this: the new guidelines do not say, “Everyone with 130/80 gets the same treatment.” They say, “Take this seriously, assess the full picture, and act early enough to reduce long-term harm.”
The lifestyle moves that actually matter
1. Follow a DASH-style eating pattern
The DASH eating plan is one of the most evidence-backed tools for lowering blood pressure. It emphasizes fruits, vegetables, whole grains, beans, nuts, lean proteins, and low-fat dairy while lowering saturated fat and sodium. It is not glamorous, but it is effective. The NHLBI also notes that keeping sodium around 1,500 mg per day can lower blood pressure even more than staying under 2,300 mg.
2. Watch sodium without becoming a spreadsheet goblin
Most people do not get most of their sodium from a dramatic salt pour at dinner. It usually comes from packaged foods, restaurant meals, deli meats, breads, soups, sauces, and snacks that pretend to be innocent. Reading labels helps. So does cooking at home more often.
3. Move your body consistently
Regular physical activity helps lower blood pressure, manage weight, and reduce stress. A solid goal is 150 minutes of moderate-intensity aerobic activity per week, or 75 minutes of vigorous activity, or a mix. Brisk walking absolutely counts. You do not need to become a mountain athlete unless that is somehow your thing.
4. Manage weight if needed
Even modest weight loss can improve blood pressure. This is not about chasing perfection. It is about lowering strain on the cardiovascular system in meaningful increments.
5. Sleep and stress are not side quests
Poor sleep, chronic stress, and conditions such as sleep apnea can all contribute to blood pressure problems. If someone tells you that you snore like a chainsaw with feelings, it may be worth bringing that up with your clinician. Blood pressure control is not just about food and exercise; it is also about recovery.
How to take your blood pressure at home without sabotaging the result
This section deserves more love than it gets because technique can dramatically change the number on the screen. Home monitoring is helpful only if you do it correctly.
- Do not smoke, drink caffeine, or exercise within 30 minutes before checking.
- Empty your bladder first.
- Sit quietly for at least five minutes.
- Keep your back supported, feet flat on the floor, and legs uncrossed.
- Place the cuff on a bare upper arm, not over clothing.
- Support your arm on a flat surface at heart level.
- Take two readings, one minute apart, and record both.
- Measure at about the same time each day.
That arm position detail is not fussy medical theater. A Johns Hopkins study found that resting the arm on the lap or leaving it unsupported at the side can falsely raise readings by several points, enough in some cases to bump a person into a higher category. So yes, your blood pressure monitor is judging your posture.
When should you worry right away?
If your reading is 180/120 mm Hg or higher, that is considered a hypertensive crisis range. If it stays that high, especially with symptoms like chest pain, shortness of breath, weakness, confusion, severe headache, trouble speaking, or vision changes, get urgent medical care. That is not a “drink some water and see what happens” situation.
For everything below that level, the smarter move is usually to measure correctly, log your readings, and talk with your clinician about trends. Blood pressure management is a long game, not a one-number morality test.
Common mistakes people make when reading the guidelines
Mistake #1: Thinking 130/80 is a panic button
It is a signal to take prevention seriously, not an automatic emergency.
Mistake #2: Assuming symptoms will warn you
High blood pressure usually has no obvious symptoms. Waiting to “feel it” is a terrible strategy.
Mistake #3: Believing medication means failure
Medication is not a moral defeat. It is one tool among several for reducing risk.
Mistake #4: Treating one reading like a final verdict
Trends matter more than a single spike. Proper measurement matters, too.
Mistake #5: Ignoring the bigger health picture
Age, diabetes, kidney disease, prior heart disease, sleep apnea, weight, family history, and overall cardiovascular risk all shape what the guidelines mean for you personally.
Conclusion: how to read the new guidelines without overreacting
The best way to read the new blood pressure guidelines is with equal parts seriousness and calm. Yes, the definition changed. Yes, 130/80 matters. Yes, the newer approach means more adults are now considered to have hypertension. But the point is not to frighten people into staring at sodium labels under fluorescent lighting. The point is to reduce damage early, confirm readings accurately, and build a plan that fits the person behind the numbers.
If your readings are normal, keep protecting that win. If they are elevated, tighten up lifestyle habits before the numbers drift higher. If you are already in Stage 1 or Stage 2, do not treat the guidelines like bad news; treat them like useful information arriving on time for once. That is rare enough to appreciate.
In plain English, Harvard Health’s framing still holds up: the guidelines are easier to understand when you stop asking, “Am I sick now?” and start asking, “What is the smartest next step for my heart, brain, and future self?” That question is far more useful than arguing with a cuff.
Experiences People Commonly Have When Reading the New Blood Pressure Guidelines
One of the most common experiences people have is simple disbelief. Someone gets a reading around 132/82, hears the phrase “Stage 1 hypertension,” and immediately thinks, “That cannot be right. I jog. I eat salad. I only panic on weekdays.” The new guidelines can feel surprisingly personal because they reclassify numbers many people once dismissed as “a little high, but probably fine.” That emotional reaction is normal. The updated categories force people to rethink what “healthy enough” really means.
Another common experience is discovering that blood pressure behaves differently depending on where and how it is measured. A person may get a high reading in a clinic, buy a home monitor in a burst of determination, then discover their numbers are lower and more consistent at home. For some, that is reassuring. For others, it is annoying in a very specific, modern way: now they own one more device that knows too much about them. Still, this is often the moment the guidelines start making sense. The numbers are not random. The conditions around the reading matter.
Many people also go through a “hidden sodium” awakening. They stop blaming the salt shaker and start noticing the real offenders: canned soup, restaurant sandwiches, frozen meals, sauces, snack foods, and the kind of “healthy” wrap that somehow contains enough sodium to season a driveway. Reading the guidelines often becomes less about abstract medicine and more about practical habits. Suddenly, grocery labels become required reading, and people realize blood pressure control lives in ordinary decisions, not just doctor visits.
There is also the experience of learning that lifestyle change is not cosmetic. For years, advice like “walk more,” “sleep better,” or “cut back on sodium” may have sounded like generic wellness wallpaper. But when people understand how these steps affect a real number tied to stroke and heart disease risk, the advice lands differently. A daily walk is no longer just a virtuous activity done by people in commercials. It becomes part of a treatment strategy.
Some readers come away with relief rather than fear. They realize the guidelines are not telling them they failed; they are giving them a clearer map. Instead of waiting until blood pressure gets worse, they have a chance to act earlier. That can feel empowering. It shifts the story from “I have a problem” to “I have useful information.” And honestly, useful information is one of the few things in adult life that deserves a standing ovation.
Finally, many people experience a mindset change. They stop thinking of blood pressure as a one-time event and start seeing it as an ongoing trend. That may be the most valuable lesson of all. The new blood pressure guidelines are not just about lower cutoffs. They are about better awareness, earlier action, and smarter prevention. Once people understand that, the numbers stop feeling like a verdict and start feeling like feedback.






