Table of Contents >> Show >> Hide
- What is sphincter of Oddi dysfunction?
- How the sphincter of Oddi works
- Sphincter of Oddi dysfunction symptoms
- Who is more likely to develop SOD?
- Types of sphincter of Oddi dysfunction
- How SOD is diagnosed
- Sphincter of Oddi dysfunction diet: What to eat and what to limit
- Relief options for sphincter of Oddi dysfunction
- When to seek medical care quickly
- Practical tips for daily relief
- Conclusion
- Experiences related to sphincter of Oddi dysfunction
- SEO Tags
Medical note: This article is for educational purposes only and does not replace diagnosis or treatment from a licensed healthcare professional. Severe abdominal pain, fever, yellowing skin or eyes, repeated vomiting, dark urine, pale stools, chest-like pain, or pain with fainting should be treated as urgent medical concerns.
What is sphincter of Oddi dysfunction?
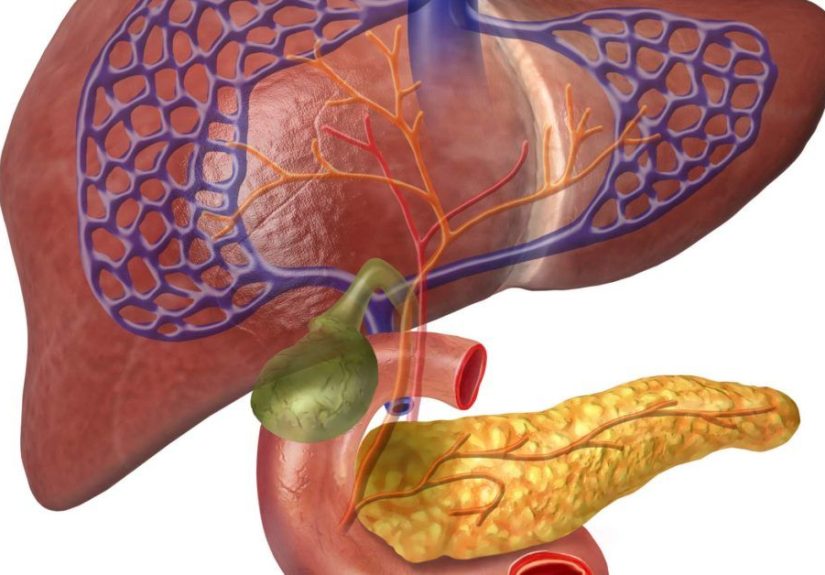
Sphincter of Oddi dysfunction, often shortened to SOD, is one of those medical terms that sounds like it was invented during a spelling contest no one wanted to attend. But the condition itself is very real. The sphincter of Oddi is a small muscular valve located where the bile duct and pancreatic duct empty into the first part of the small intestine, called the duodenum. Its job is simple but important: open at the right time, let bile and pancreatic juices flow through, then close again.
When the sphincter does not relax properly, becomes too tight, or spasms, digestive fluids can back up. That backup may create pressure in the bile duct or pancreatic duct, leading to upper abdominal pain that can feel a lot like a gallbladder attack. Many people hear about sphincter of Oddi dysfunction after gallbladder removal, especially when pain continues even though the gallbladder has already made its dramatic exit.
SOD is uncommon, difficult to diagnose, and sometimes misunderstood. It can overlap with other digestive problems such as gallstones, bile duct stones, pancreatitis, ulcers, acid reflux, irritable bowel syndrome, functional abdominal pain, and liver or pancreatic disease. That is why the best approach is not guessing, Googling at 2 a.m., and blaming your last taco. It is careful evaluation by a gastroenterologist.
How the sphincter of Oddi works
To understand SOD, picture your digestive system as a kitchen with several hardworking appliances. The liver makes bile, which helps digest fat. The gallbladder stores bile, although people can live without it. The pancreas makes enzymes that help break down food. The sphincter of Oddi acts like a tiny gatekeeper, controlling when those fluids enter the intestine.
During normal digestion, the gate opens smoothly. With sphincter of Oddi dysfunction, the gate may clamp down, open poorly, or become narrowed from scarring or inflammation. As pressure builds, pain can follow. In some cases, the backup mainly affects the bile ducts. In others, it involves the pancreatic duct and may be linked with pancreatitis.
Sphincter of Oddi dysfunction symptoms
The classic symptom of sphincter of Oddi dysfunction is recurring upper abdominal pain. The pain is often felt in the right upper abdomen or the center upper abdomen, just below the ribs. It may spread to the back, right shoulder, or shoulder blade area. People often describe it as sharp, squeezing, deep, pressure-like, or “gallbladder pain without a gallbladder.”
Common SOD symptoms include:
- Severe pain in the upper right or upper middle abdomen
- Pain that may radiate to the back or right shoulder
- Episodes lasting 30 minutes or longer
- Nausea or vomiting during attacks
- Pain after eating, especially after fatty meals
- Bloating or indigestion-like discomfort
- Temporary abnormal liver enzymes during attacks
- Pancreatitis-like symptoms in pancreatic-type SOD
One frustrating feature of SOD is that tests may look normal between attacks. A person may feel terrible on Tuesday, finally get labs on Thursday, and be told everything is “fine.” That does not mean the pain is imaginary. It means timing, pattern recognition, and the right diagnostic strategy matter.
Who is more likely to develop SOD?
Sphincter of Oddi dysfunction is most often discussed in people who have had their gallbladder removed, a surgery called cholecystectomy. After gallbladder removal, bile flows more directly from the liver into the small intestine. Most people do well, but some continue to have biliary-type pain. In a smaller group, the sphincter of Oddi may be part of the problem.
Risk may also be higher in people with a history of pancreatitis, bile duct procedures, inflammation near the ducts, or certain anatomical or motility issues. Some medications that affect biliary pressure or intestinal movement may worsen symptoms in susceptible people, so it is important to review all prescriptions, over-the-counter drugs, and supplements with a clinician.
Types of sphincter of Oddi dysfunction
Historically, doctors divided SOD into types based on symptoms, lab results, and bile duct findings. Modern gastroenterology has moved toward more precise language, especially because not all unexplained post-gallbladder pain benefits from invasive treatment.
Biliary sphincter disorder
This type involves biliary-type pain, meaning pain that resembles gallbladder or bile duct pain. It may come with temporary liver enzyme elevations or a dilated bile duct when no stone, tumor, or structural blockage is found. The pain is usually strong enough to interrupt daily activity and is not explained by bowel movements, posture, or antacids.
Pancreatic sphincter disorder
This type is suspected when the pancreatic duct is involved, especially in people with recurrent pancreatitis or pancreatic enzyme elevations. Pancreatic-type SOD requires careful specialist evaluation because procedures around the pancreatic duct can carry a higher risk of complications.
Functional abdominal pain that mimics SOD
Some people have upper abdominal pain that feels biliary but does not show objective signs of bile duct obstruction or pancreatic involvement. This group is especially important because invasive procedures such as ERCP and sphincterotomy may not help and can cause harm. Pain can still be real and severe, but the treatment plan may focus more on noninvasive management, pain modulation, diet, and ruling out other conditions.
How SOD is diagnosed
Diagnosing sphincter of Oddi dysfunction is not like diagnosing a broken arm. There is no simple “yep, there it is” moment on a standard X-ray. Doctors usually begin by excluding more common and dangerous causes of upper abdominal pain.
Tests doctors may consider
- Blood tests: Liver enzymes, bilirubin, amylase, and lipase may be checked, especially during or soon after pain episodes.
- Ultrasound: This can look for bile duct dilation, stones, liver problems, or other abnormalities.
- MRCP: Magnetic resonance cholangiopancreatography uses MRI technology to view bile and pancreatic ducts without an endoscope.
- Endoscopic ultrasound: This may help detect small stones, sludge, pancreatic disease, or duct problems missed by other imaging.
- HIDA scan or biliary scintigraphy: In selected cases, this may help assess bile flow.
- ERCP with manometry: This is an invasive test that measures sphincter pressure, but it is used far more cautiously today because of risks.
The most important point: ERCP is not just a diagnostic camera ride. It is an advanced endoscopic procedure with a meaningful risk of pancreatitis, especially in people suspected of having SOD. For that reason, many specialists reserve ERCP for carefully selected patients with objective evidence of obstruction or recurrent pancreatitis.
Sphincter of Oddi dysfunction diet: What to eat and what to limit
Diet does not “cure” sphincter of Oddi dysfunction, but it may reduce symptom flares for some people. Because bile is heavily involved in fat digestion, high-fat meals can be a common trigger. The goal is not to live on plain rice and sadness. The goal is to make digestion easier while keeping meals balanced and enjoyable.
Foods that may help
- Lean proteins such as skinless chicken, turkey, fish, egg whites, tofu, and beans if tolerated
- Low-fat dairy or dairy alternatives
- Oatmeal, brown rice, quinoa, whole-grain toast, and other gentle high-fiber carbohydrates
- Cooked vegetables, especially during sensitive periods
- Fruits such as bananas, applesauce, berries, melon, and pears
- Small amounts of healthy fats, spread throughout the day rather than eaten in one heavy meal
- Water, herbal tea, and noncarbonated drinks if carbonation worsens bloating
Foods and habits that may trigger symptoms
- Fried foods, fast food, heavy cream sauces, and greasy meats
- Large meals that stretch the stomach and demand a big digestive response
- Alcohol, especially in people with pancreatic symptoms or pancreatitis risk
- Very spicy foods, if they worsen pain or reflux
- Large desserts, pastries, and high-fat snacks
- Skipping meals all day and then eating one huge dinner
A simple SOD-friendly meal example
Breakfast might be oatmeal with banana and a small spoonful of nut butter. Lunch could be grilled chicken, rice, and steamed carrots. Dinner might be baked fish with sweet potato and green beans. Snacks could include low-fat yogurt, applesauce, toast, or a smoothie made with low-fat ingredients. This is not glamorous, but neither is arguing with your bile duct at midnight.
A food diary can be surprisingly useful. Track meals, fat content, timing, pain level, nausea, bowel changes, medications, stress, and sleep. Patterns often appear after two to four weeks. For example, one person may tolerate avocado but not fried chicken, while another reacts to large meals more than specific foods.
Relief options for sphincter of Oddi dysfunction
Relief depends on the type of SOD, the severity of symptoms, test results, and whether the bile duct, pancreatic duct, or both are involved. Treatment should be individualized. What helps one person may do absolutely nothing for another, because digestive systems love being dramatic and inconsistent.
1. Low-fat, smaller meals
Many patients start with a lower-fat eating pattern and smaller, more frequent meals. This may reduce the intensity of bile flow demands after eating. It is especially useful for people who notice pain after rich meals, fried foods, or restaurant food.
2. Avoid alcohol and smoking
Alcohol can increase pancreatic stress and may worsen pancreatitis risk. Smoking is also linked with poorer digestive and pancreatic health. Avoiding both is a practical step, particularly for people with pancreatic-type symptoms.
3. Medication options
Doctors may consider medications that relax smooth muscle, reduce spasms, manage nausea, or treat overlapping functional pain. Options sometimes discussed include antispasmodics, calcium channel blockers, nitrates, non-opioid pain relievers, or medications that calm nerve-related gut pain. These should only be used under medical supervision because side effects and interactions matter.
4. Treating overlapping digestive problems
Reflux, gastritis, ulcers, constipation, bile acid diarrhea, pancreatic insufficiency, and irritable bowel syndrome can all create symptoms that overlap with SOD. Treating these conditions may reduce the total pain burden, even if the sphincter is still part of the story.
5. ERCP and sphincterotomy
In carefully selected cases, a specialist may recommend ERCP with sphincterotomy. During sphincterotomy, the sphincter is cut to improve drainage. This may help certain patients with objective signs of obstruction, such as abnormal liver tests, duct dilation, or recurrent pancreatitis. However, it is not a casual procedure. ERCP can cause pancreatitis, bleeding, infection, and perforation. Modern care is more selective because research has shown that patients with pain alone and no objective abnormalities may not benefit from sphincterotomy.
When to seek medical care quickly
Upper abdominal pain should not automatically be labeled as SOD. Some symptoms require prompt medical attention because they may signal infection, pancreatitis, bile duct obstruction, heart problems, or another urgent condition.
- Severe or worsening abdominal pain
- Fever or chills
- Yellow skin or eyes
- Dark urine or pale stools
- Repeated vomiting or inability to keep fluids down
- Confusion, fainting, or weakness
- Chest pressure, shortness of breath, or pain spreading to the jaw or left arm
Practical tips for daily relief
Living with suspected or diagnosed sphincter of Oddi dysfunction often means learning how to reduce flares, communicate clearly with doctors, and avoid unnecessary procedures. Start by documenting symptoms in a structured way. Write down when pain starts, where it is located, how long it lasts, what you ate, and whether nausea, vomiting, fever, or jaundice occurred.
Ask your doctor whether labs should be drawn during an attack, because liver enzymes and pancreatic enzymes may be more revealing during symptoms than days later. Keep copies of imaging reports, surgical notes from gallbladder removal, ERCP reports, and lab trends. Digestive cases can become complicated, and having organized records saves everyone from playing medical detective with half the clues missing.
Gentle movement, stress reduction, heat packs, hydration, and regular sleep may not fix the sphincter itself, but they can help lower the body’s overall pain sensitivity. Chronic abdominal pain often becomes a full-body experience. The gut, brain, nervous system, and stress response are all in the group chat.
Conclusion
Sphincter of Oddi dysfunction is a complex digestive disorder involving the small muscular valve that controls the flow of bile and pancreatic juices into the small intestine. The main symptom is recurring upper abdominal pain, often after meals and sometimes after gallbladder removal. A low-fat diet, smaller meals, alcohol avoidance, food tracking, and careful medical evaluation may help reduce symptoms. Invasive procedures such as ERCP and sphincterotomy can help selected patients, but they are not the right answer for everyone and should be approached with caution.
The smartest path is balanced: take symptoms seriously, rule out more common causes, use diet and lifestyle strategies where helpful, and work with a gastroenterologist who understands modern SOD diagnosis and treatment. In other words, do not ignore the painbut do not let your sphincter of Oddi bully you into panic-scrolling forever, either.
Experiences related to sphincter of Oddi dysfunction
People who deal with sphincter of Oddi dysfunction often describe the experience as confusing before it is painfuland then very painful. A common story begins after gallbladder removal. The patient expects life to improve, and at first it may. Then, weeks or months later, a familiar upper-right abdominal pain returns. The gallbladder is gone, but the “gallbladder attack” feeling seems to have left a forwarding address.
One typical experience involves pain after a heavy meal. Someone eats fried chicken, buttery potatoes, or a creamy pasta dish and feels fine for a short time. Then pressure builds under the ribs. The discomfort sharpens, wraps toward the back, and brings nausea along like an unwanted dinner guest. The person may try antacids, stretching, walking, or lying down, but the pain follows its own schedule. After 45 minutes, two hours, or sometimes longer, it fades. By the time they get medical help, tests may be normal, which can feel incredibly discouraging.
Another common experience is the “normal test, abnormal life” problem. A person may have an ultrasound, CT scan, endoscopy, blood work, and still not get a clear answer. They may be told it is reflux, stress, IBS, scar tissue, or “just digestion.” Sometimes those explanations are correct. Sometimes they are incomplete. This is why symptom timing matters. If liver enzymes or pancreatic enzymes rise during attacks, that information can change the conversation with a gastroenterologist.
Many people also learn that diet is not a magic switch, but it can be a useful dimmer. A strict low-fat diet may reduce attacks for some, while others only need to avoid the biggest triggers: fried food, alcohol, oversized meals, and rich desserts. Some patients find that eating five smaller meals works better than three large meals. Others discover that stress, poor sleep, and dehydration make their digestive system more reactive. The lesson is not that symptoms are “all in your head.” The lesson is that the digestive tract listens to everythingfood, hormones, nerves, sleep, and stressand sometimes it listens with a megaphone.
The emotional side of SOD deserves attention too. Recurrent pain can make people afraid to eat, travel, attend social events, or make plans. Restaurant menus become strategy documents. Family dinners may come with quiet calculations: How much fat is in this? How far is the bathroom? Will I be in pain on the drive home? These worries are understandable, but they should not be faced alone. A good care plan may include a gastroenterologist, dietitian, primary care clinician, and, when pain becomes chronic, a pain specialist or therapist familiar with gut-brain disorders.
For many patients, relief is not one dramatic cure but a series of practical wins: fewer attacks, shorter flares, clearer triggers, better communication with doctors, and confidence about when to seek urgent care. SOD can be stubborn, but with careful evaluation and a realistic plan, many people regain control over meals, routines, and quality of life.






