Table of Contents >> Show >> Hide
- What “Contracted” (or “Collapsed”) Gallbladder Actually Means
- Symptoms: What You Might Feel (and What It Can Be Mistaken For)
- What Causes a Contracted Gallbladder?
- Diagnosis: How Doctors Figure Out What’s Going On
- Treatment: What Helps Depends on the Cause
- Food, Lifestyle, and Prevention: What Actually Makes a Difference
- What to Ask Your Clinician If Your Report Says “Contracted Gallbladder”
- FAQ
- Conclusion
- Experiences: What People Commonly Report (and What It’s Like in Real Life)
- The ultrasound-prep plot twist: “They couldn’t see it… so I had to redo the test.”
- The classic gallbladder-attack experience: “It felt like a stubborn pain that wouldn’t move.”
- The pattern recognition phase: “I didn’t connect the dots until the third time.”
- When the plan becomes surgery: nerves, relief, and a surprisingly normal life after
- Practical tips people say helped (not medical ordersjust common sense themes)
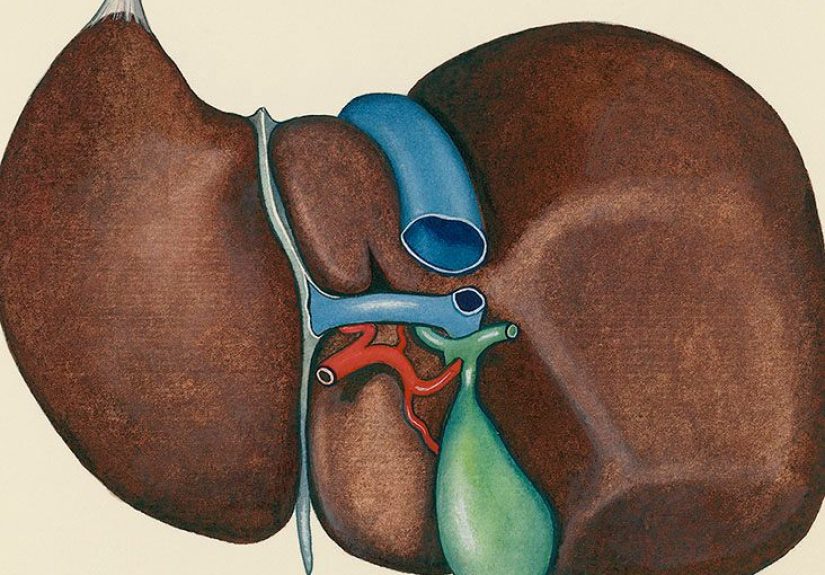
Your gallbladder is basically your liver’s tiny “bile pantry.” It stores bile (a digestive fluid) and squeezes it into your small intestine when you eat,
especially when you eat fat. So here’s the plot twist: a “contracted” gallbladder isn’t automatically a problemsometimes it’s just doing its job.
The tricky part is figuring out when a contracted (or “collapsed”) gallbladder is normal… and when it’s a sign of gallbladder disease.
In everyday medical language, collapsed and contracted gallbladder usually mean the gallbladder looks small or not well-distended
on imaging (most often ultrasound). That can happen because you ate too recently (normal physiology), or because inflammation and scarring have made the
gallbladder stiff and shrunken (often related to gallstones and chronic cholecystitis). The symptoms and treatment depend on the “why,” not just the word
on the report.
What “Contracted” (or “Collapsed”) Gallbladder Actually Means
1) The normal (and very boring) reason: you weren’t fasting
After you eat, your body releases hormones that tell the gallbladder to squeeze bile out. That squeeze makes it look smallersometimes so small that an
ultrasound report may say it’s “contracted” or even “not well visualized.” That’s why many imaging centers ask you to fast before a right-upper-quadrant
or abdominal ultrasound: they want the gallbladder relaxed and filled with bile so it’s easier to evaluate.
2) The not-so-boring reason: chronic gallbladder disease
If the gallbladder stays small even when you’ve fasted properly, it can suggest a “non-distending” or chronically diseased gallbladder. A common pathway:
gallstones irritate the gallbladder over time, leading to chronic inflammation (chronic cholecystitis). The gallbladder wall can thicken,
scar tissue can build up, and the organ may shrink and lose flexibility. In some cases, the gallbladder can be packed with stones, producing classic
ultrasound patterns that make it hard to see the normal fluid-filled shape.
3) Other possibilities (less common, but worth knowing)
- Acute cholecystitis (active inflammation), often triggered by a stone blocking the cystic duct.
- Functional gallbladder disorders (like biliary dyskinesia), where contraction/ejection isn’t coordinated or effective.
- Bile duct blockage (for example, a stone in the common bile duct), which changes pressures and bile flow.
- Technical/visibility issues during ultrasound (bowel gas, anatomy, positioning).
- History of gallbladder removal (sounds obvious, but it comes up in “nonvisualized gallbladder” discussions).
- Congenital absence of the gallbladder (rare, but real).
Symptoms: What You Might Feel (and What It Can Be Mistaken For)
Some people with a contracted gallbladder have no symptomsespecially if the “contraction” was simply because they ate beforehand.
When symptoms do show up, they usually reflect the underlying problem (most commonly gallstones or inflammation).
Common symptoms linked to gallstones or gallbladder inflammation
- Right upper abdominal pain (or pain in the upper middle abdomen) that can last 30 minutes to several hours.
- Pain after meals, especially heavy or fatty meals; it may show up later in the day or at night.
- Pain that radiates to the right shoulder or back.
- Nausea and vomiting.
- Bloating, indigestion-like discomfort, or feeling “off” after eating (less specific, but common complaints).
Red-flag symptoms that should be treated as urgent
Gallbladder issues can overlap with many other conditions (acid reflux, ulcers, liver problems, even cardiac pain). But these symptoms deserve prompt
medical attention because they can signal complications like infection, bile duct obstruction, or pancreatitis:
- Fever or chills with abdominal pain
- Jaundice (yellowing of skin/eyes), dark urine, or clay-colored stools
- Severe pain lasting more than a few hours or pain that keeps escalating
- Persistent vomiting or inability to keep fluids down
- Confusion, weakness, or signs of dehydration
What Causes a Contracted Gallbladder?
Gallstones (the main character in most gallbladder stories)
Gallstones are hardened particles (often cholesterol-based, sometimes pigment stones) that can form in the gallbladder. Many people have “silent”
gallstones, but when stones block bile flow, they can trigger painful attacks and inflammation. Repeated irritation can lead to chronic scarring and a
smaller, less flexible gallbladder.
Chronic cholecystitis (slow-burn inflammation)
Chronic cholecystitis often develops after repeated gallstone-related episodes. The gallbladder may become thick-walled and contracted over time. People
might describe recurring right-upper-quadrant pain after meals, recurring nausea, or “attacks” that come and go.
Acute cholecystitis (fast, angry inflammation)
Acute cholecystitis is typically triggered by a stone blocking the cystic duct, trapping bile and causing swelling and inflammation. It’s often more
intense, may include fever, and commonly requires urgent evaluation.
Biliary dyskinesia or functional gallbladder disorder
Sometimes the gallbladder isn’t working right even without stones. In biliary dyskinesia, the gallbladder’s contraction and bile ejection can be
ineffective, leading to biliary-type pain. A functional test (often a HIDA scan with ejection fraction) may be used when ultrasound doesn’t show stones.
Diagnosis: How Doctors Figure Out What’s Going On
Step 1: History + exam
The details matter: when pain happens, whether it’s linked to meals, how long it lasts, whether you have fever or jaundice, and what makes it better or
worse.
Step 2: Blood tests (when needed)
Bloodwork can help look for signs of inflammation/infection and check liver and pancreas-related markersespecially if symptoms suggest complications or
bile duct involvement.
Step 3: Imaging (where “contracted gallbladder” shows up)
-
Ultrasound: Often the first test for gallbladder symptoms. It can detect gallstones and signs of inflammation (like wall thickening or
fluid around the gallbladder). -
Repeat ultrasound after proper fasting: If the gallbladder looks contracted because you ate recently, repeating the test with correct
prep can clarify. -
HIDA scan (cholescintigraphy): A nuclear medicine test that evaluates bile flow and gallbladder function. It can help diagnose
cholecystitis and assess gallbladder ejection in suspected functional disorders. - CT or MRI/MRCP: Sometimes used to look for complications or evaluate bile ducts and surrounding structures.
-
ERCP: A specialized procedure primarily used when a bile duct stone or obstruction is suspected (and treatment may be performed during
the procedure).
Treatment: What Helps Depends on the Cause
If it’s contracted because you ate (normal)
Treatment may be as simple as: “Nope, you’re finejust repeat the ultrasound with the correct fasting instructions.” If you had no symptoms and the only
finding is a contracted gallbladder after eating, it’s often not a diagnosis by itself.
If gallstones are causing symptoms (biliary colic)
Symptomatic gallstones are a common reason for elective gallbladder removal (cholecystectomy). During an acute pain episode, clinicians
focus on pain control and evaluating for complications. Long-term, surgery is often the definitive fix for recurrent attacks.
If acute cholecystitis is suspected
Acute cholecystitis typically requires prompt medical evaluation. Treatment may include IV fluids, pain control, and antibiotics if infection is suspected.
Many cases ultimately require cholecystectomy (often laparoscopic), sometimes urgently depending on severity and timing.
If chronic cholecystitis has led to a contracted gallbladder
When symptoms are recurrent and imaging suggests chronic gallbladder disease, elective laparoscopic cholecystectomy is commonly recommended. People often
worry that life without a gallbladder will be a digestive disaster. In reality, many do wellbile simply flows directly from the liver into the intestine.
Some people have temporary loose stools after surgery, which usually improves with time and diet adjustments.
If biliary dyskinesia is suspected
If symptoms are classic for gallbladder pain but ultrasound doesn’t show stones, clinicians may use a HIDA scan to evaluate gallbladder function.
Treatment decisions are individualizedespecially because abdominal pain can have many causes and test results need to match symptoms.
Food, Lifestyle, and Prevention: What Actually Makes a Difference
Diet changes that can reduce symptom flare-ups
- Go easier on very fatty meals if they trigger pain (fried foods, heavy cream sauces, giant cheese-loaded portions).
- Try smaller, more frequent meals if large meals reliably set you off.
- Choose fiber-rich foods (fruits, vegetables, whole grains) for overall metabolic and digestive healthgo slowly if you’re sensitive.
- Stay hydrated and aim for steady routines (wild meal-skipping can be unhelpful for gallstone risk in some people).
Weight changes: slow is smoother
Rapid weight loss is associated with gallstone risk. If weight loss is a goal, gradual changes are generally preferred over crash dieting. (Your gallbladder
likes stability. It’s not emotionally expressive, but it’s picky.)
What to Ask Your Clinician If Your Report Says “Contracted Gallbladder”
- Was I properly fasting for the ultrasound? If not, should the test be repeated with correct prep?
- Did the ultrasound show gallstones, gallbladder wall thickening, or fluid around the gallbladder?
- Do my symptoms fit biliary colic, cholecystitis, reflux, ulcers, or something else?
- Do I need blood tests to check liver enzymes, infection markers, or pancreas markers?
- Should I have a HIDA scan to evaluate function if ultrasound was normal but symptoms persist?
- If surgery is recommended: laparoscopic vs open, expected recovery, and how to manage diet afterward?
FAQ
Is a contracted gallbladder always serious?
No. It can be completely normal after eating. It becomes more meaningful if you were fasting and/or you have symptoms consistent with gallbladder disease.
Can a contracted gallbladder cause pain by itself?
The contraction itself is a normal process. Pain usually comes from an underlying issuecommonly stones blocking flow, inflammation, or a functional
disorder.
Do you need surgery for a contracted gallbladder?
Not automatically. Surgery is typically considered when there are recurrent symptoms, gallstones, inflammation, or evidence that the gallbladder is
chronically diseased.
What happens if you remove the gallbladder?
Bile still reaches your intestines, but it flows more continuously instead of being stored and released in bursts. Many people return to normal diets over
time. Some experience temporary diarrhea or sensitivity to fatty foods during the adjustment period.
Conclusion
A “collapsed” or “contracted” gallbladder can mean two very different things: a normal gallbladder doing its post-meal squeeze, or a gallbladder that has
become stiff and shrunken from chronic disease. The smartest next step is to connect the imaging finding to real life: Were you fasting? What symptoms do
you have? And do labs or additional imaging suggest gallstones, inflammation, or a functional problem?
If you have recurrent right-upper-quadrant painespecially with nausea, fever, or jaundicedon’t self-diagnose via internet archaeology. Get evaluated.
Gallbladder problems are common, and the good news is that effective treatments (including minimally invasive surgery when appropriate) are widely available.
Experiences: What People Commonly Report (and What It’s Like in Real Life)
The phrase “contracted gallbladder” often shows up in one of two very relatable storylines: the ultrasound-prep plot twist and the
why-does-dinner-hate-me plot twist.
The ultrasound-prep plot twist: “They couldn’t see it… so I had to redo the test.”
A surprisingly common experience is going for an abdominal ultrasound and later hearing: “Your gallbladder was contracted” or “not well visualized.”
People then replay their morning like a detective: “Waitwas that latte ‘food’?” (Often, yes. The gallbladder is dramatic about calories.) Many end up
repeating the ultrasound after a proper fast, and the gallbladder suddenly becomes much easier to assess. The emotional arc here is usually:
inconvenience → mild annoyance → relief when the follow-up gives clearer answers.
The classic gallbladder-attack experience: “It felt like a stubborn pain that wouldn’t move.”
When gallstones or gallbladder inflammation are involved, people often describe pain that builds into a steady, intense discomfort in the right upper
abdomen or upper middle abdomen. It’s not always a sharp “stab”sometimes it’s a strong pressure or deep ache that refuses to be ignored. A frequent detail:
it tends to show up after a heavier meal (think pizza, burgers, creamy pasta, or fried foods). Some people notice it radiates into the back or right
shoulder, which can feel weirdly unfairlike their gallbladder is filing complaints in multiple departments.
The pattern recognition phase: “I didn’t connect the dots until the third time.”
A lot of folks don’t realize it might be gallbladder-related until there’s a pattern: pain after meals, nausea, maybe an episode late at night, then a
stretch of normal days. Because symptoms can mimic reflux or “indigestion,” many try antacids first. Some report that over-the-counter remedies help
minimally (or not at all) when the core issue is bile flow obstruction or inflammation.
When the plan becomes surgery: nerves, relief, and a surprisingly normal life after
If cholecystectomy is recommended, people often feel two things at once: nervous about surgery and relieved that there’s a clear fix. After laparoscopic
surgery, many describe a short-term “reset” periodeating lighter meals, reintroducing fats slowly, and learning which foods their body forgives quickly.
A common short-term complaint is loose stools or urgency, especially after greasy foods. For many, this improves over weeks to months, and they’re back to
normal routines with far fewer pain episodesoften none.
Practical tips people say helped (not medical ordersjust common sense themes)
- Keeping a food-and-symptom note for a couple of weeks to spot triggers.
- Choosing lower-fat meals during active symptom periods (less gallbladder “demand”).
- Taking ultrasound prep seriously to avoid repeat appointments.
- Knowing the red flags (fever, jaundice, worsening pain) and not waiting them out.
The big takeaway from these experiences: the words on an imaging report matter less than the full picturesymptoms, timing, test prep, and whether there’s
evidence of stones or inflammation. When everything is lined up correctly, people often go from “mystery pain” to a clear diagnosis and a manageable plan.





