Table of Contents >> Show >> Hide
- What Was Found in the United States?
- What Is Drug-Resistant Ringworm, Exactly?
- Why Doctors Are Paying Attention
- How Drug-Resistant Ringworm Spreads
- Why Resistance May Be Growing
- Symptoms That Deserve a Closer Look
- How It Is Treated
- Prevention Without Panic
- Real-World Experiences: What Patients Go Through When Ringworm Becomes a Long Haul
- The Bigger Takeaway
Ringworm has always had a branding problem. It sounds like a creepy-crawly pest, but it is actually a fungal infection, not a worm at all. Usually, it is annoying rather than headline-worthy: a scaly rash, some itching, a trip to the pharmacy, done. But the first confirmed U.S. cases of drug-resistant ringworm changed that script. Suddenly, a condition many people think of as a mild skin nuisance started looking more like a warning flare from the world of antimicrobial resistance.
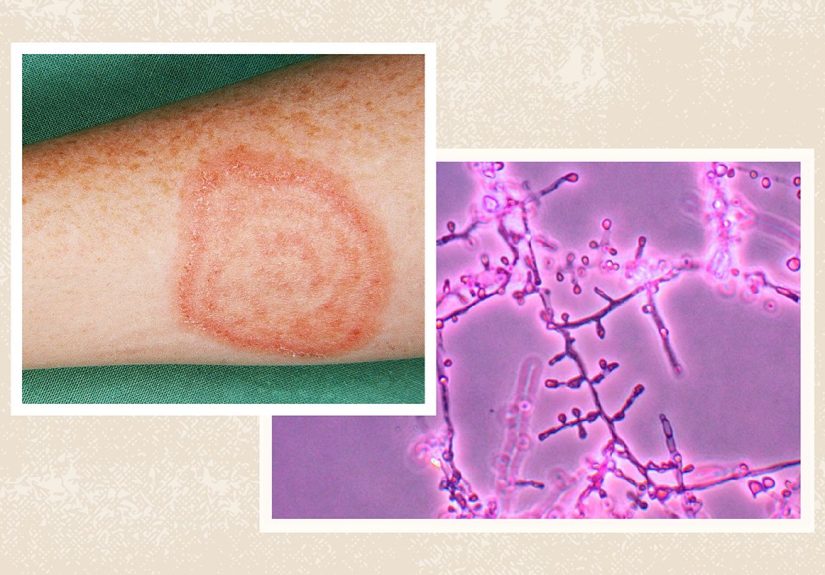
The fungus at the center of the story is Trichophyton indotineae, an emerging dermatophyte linked to severe, highly contagious, and often stubborn skin infections. It has been associated with ringworm that does not respond well to terbinafine, one of the most commonly used oral antifungal drugs. In other words, this is not your garden-variety rash that politely packs up after a tube of cream and a pep talk.
Why does this matter? Because ringworm is common, spreads easily, and can be misdiagnosed. When a harder-to-treat strain shows up in the United States, it raises concerns not just for dermatologists, but for primary care doctors, urgent care clinics, families, athletes, and anyone who has ever borrowed a towel at the gym and immediately regretted all life choices.
What Was Found in the United States?
The first confirmed U.S. cases of ringworm caused by T. indotineae were reported in New York City in 2023. The two initial patients were adult women with widespread, itchy, scaly rashes that did not improve with terbinafine, a first-line oral treatment for many tinea infections. One of the most striking details in the CDC report was that one patient had no recent international travel history, suggesting local transmission may already have been happening inside the United States.
That finding turned what could have been filed under “rare imported infection” into something far more important. If a resistant fungus can spread locally, clinicians can no longer assume the problem exists only overseas or only in travelers. Later reports strengthened that concern. Researchers in New York City described a larger group of patients with confirmed T. indotineae infections, many of whom had widespread lesions, long diagnostic delays, and failed standard antifungal treatment before finally getting the right diagnosis.
In short, the first cases were not a one-off curiosity. They were more like the opening scene of a medical mystery that already had extra chapters waiting in the wings.
What Is Drug-Resistant Ringworm, Exactly?
Ringworm, also called tinea or dermatophytosis, is a fungal infection that affects the skin, scalp, nails, groin, feet, beard area, or other body sites. It often appears as a round or ring-shaped rash, though not always. The culprit fungi feed on keratin, which is found in skin, hair, and nails. Charming houseguests, really.
Drug-resistant ringworm means the infection does not respond as expected to antifungal treatment. With T. indotineae, the big issue is frequent resistance to terbinafine. That matters because terbinafine is commonly prescribed for more widespread or stubborn infections. When that standard therapy fails, treatment gets more complicated, longer, and sometimes more expensive.
Researchers have linked this resistance to genetic mutations, including changes in the fungus’s squalene epoxidase gene. That mutation can make it harder for terbinafine to do its job. Translation: the fungus has learned how to dodge one of medicine’s favorite punches.
Why Doctors Are Paying Attention
Most ordinary ringworm infections can still be treated successfully. That is the good news, and it is worth saying clearly. The problem is that T. indotineae often looks different from the “classic” neat little ring many people expect. The rash may be widespread, inflamed, intensely itchy, and located on the trunk, groin, buttocks, thighs, face, or multiple body sites at once.
Because the infection can resemble eczema, psoriasis, contact dermatitis, or other inflammatory rashes, some patients are initially given steroid creams. That is a bad detour. Steroids can make fungal infections worse, blur the appearance of the rash, and delay the right diagnosis. It is the dermatology version of trying to fix a leaky pipe with whipped cream.
Clinicians are also concerned because testing is not simple. Many routine clinical laboratories cannot reliably distinguish T. indotineae from other, more familiar dermatophytes. Confirming the species generally requires specialized molecular testing such as genomic or internal transcribed spacer sequencing. In plain English: many doctors may suspect something odd is going on, but proving exactly what it is can take extra time and specialized labs.
That testing gap matters. A CDC survey of U.S. infectious disease specialists found that awareness of antifungal-resistant dermatophyte infections was still incomplete, and many clinicians were unsure how to obtain testing for species identification or antifungal resistance. That means some cases may be missed, misclassified, or recognized later than they should be.
How Drug-Resistant Ringworm Spreads
Like ordinary ringworm, resistant ringworm spreads through skin-to-skin contact, shared personal items, contaminated surfaces, and sometimes infected animals. Towels, bedding, clothing, locker room floors, and close-contact living arrangements can all help the fungus move from one host to the next. Infections can also spread from one part of the body to another.
That helps explain why households can become mini transmission hubs. In one of the early U.S. reports, family members of an infected patient were also being evaluated for similar rashes. Once a contagious fungal infection gets into a home, it does not exactly sit quietly in a corner reading a magazine.
Travel has also played a role in several reported cases, especially travel connected to South Asia, where T. indotineae became a major public health concern over the past decade. But travel is not the whole story anymore. Later U.S. case reports and expert commentary suggest community spread is possible, which is why American clinicians are being urged to look beyond travel history alone.
Why Resistance May Be Growing
Experts have pointed to several likely drivers. One major concern is the misuse of topical combination creams that mix antifungals with corticosteroids and sometimes antibiotics. These products may temporarily reduce redness or itching, making people think the rash is improving, while the fungus continues thriving underneath. That creates ideal conditions for prolonged infection, delayed diagnosis, and possibly resistance.
Other contributors may include inappropriate antifungal prescribing, overuse of medications without testing, incomplete treatment courses, and poor adherence. Antifungal resistance does not usually make front-page news the way antibiotic resistance does, but it follows a similar logic: the more microbes are exposed to poorly targeted or poorly used drugs, the more likely some survive and adapt.
Researchers in North America have also found that terbinafine resistance is not limited to T. indotineae. Resistant strains of T. rubrum, a more common cause of ringworm and nail infections, have also been identified. That broadens the conversation from one exotic-sounding fungus to a bigger concern about dermatophyte resistance in general.
Symptoms That Deserve a Closer Look
Most people do not need to panic over every itchy patch of skin. But some symptoms should push drug-resistant ringworm higher on the list of possibilities. These include:
Widespread rash
If lesions cover large areas of the trunk, thighs, buttocks, groin, or face, that is more concerning than a small isolated patch.
Severe itch and inflammation
Patients with T. indotineae often report intense itching, scaling, and persistent discomfort.
Treatment failure
If the rash does not improve with typical topical antifungals or oral terbinafine, clinicians may need to reconsider the diagnosis and the organism involved.
Repeated misdiagnosis
A rash treated as eczema, allergic dermatitis, or “just irritation” for months deserves a second look, especially if steroid creams seem to make it worse.
How It Is Treated
Treatment depends on the severity of infection, body site, prior therapy, and access to testing. For ordinary skin ringworm, topical antifungals often work well. But emerging resistant infections are a different beast. In difficult cases, oral therapy is often needed, and that therapy may need to continue for six to eight weeks or longer.
Itraconazole is commonly used by many clinicians as a first-line option for confirmed or strongly suspected T. indotineae because terbinafine frequently fails. However, itraconazole is not a simple plug-and-play fix. It has important drug interactions, absorption issues, and potential side effects, including liver concerns. Some patients may need monitoring, insurance wrangling, or both. Nothing says “modern health care adventure” quite like prior authorization for a fungus.
Higher-dose terbinafine has been tried in some patients, but it has not shown consistent success. Griseofulvin and fluconazole are generally not considered top options for this organism, although they may still help in select cases. The bottom line is that drug-resistant ringworm is treatable, but not casually, and definitely not with random leftover cream from the bathroom cabinet.
Prevention Without Panic
The emergence of resistant ringworm does not mean everyone should start side-eyeing every yoga mat. It does mean basic prevention deserves more respect than it usually gets. Good hygiene, not sharing towels or clothing, washing bedding on high heat, wearing footwear in locker rooms, treating infected pets, and seeking medical advice for persistent rashes all remain smart steps.
Just as important, people should avoid using over-the-counter steroid creams on undiagnosed rashes. If a rash is fungal, steroids can make the infection harder to recognize and harder to clear. When in doubt, get the rash checked before launching a one-person science experiment on your skin.
Real-World Experiences: What Patients Go Through When Ringworm Becomes a Long Haul
One of the most revealing parts of the U.S. reports is not just the microbiology. It is the human experience. Patients with drug-resistant ringworm often do not have a quick, tidy story. They have a long one.
For some, it starts with what looks like a common rash: itchy, circular, maybe annoying but manageable. Then it spreads. It moves from one patch to several. It shows up on the thighs, buttocks, abdomen, groin, or face. The itching gets stronger. Clothing rubs the skin and makes everything worse. Sleep becomes harder. The person tries a cream, then another cream, then an urgent care visit, then a different prescription. Nothing really works.
That cycle of near-improvement and disappointment can stretch for months. In the New York City case series, patients experienced diagnostic delays ranging from a few months to well over a year. During that time, some were treated with topical antifungals that did not help, while others received therapies that were not quite right for the actual organism involved. It is easy to imagine the frustration: every new tube or pill comes with hope, and every treatment failure makes the next promise sound less convincing.
There is also the social side of the experience. Ringworm is visible. It can affect intimate areas. It can be mistaken for poor hygiene, even though anyone can get it. Patients may feel embarrassed discussing rashes on the groin, buttocks, or pubic region, which delays care even more. Some may avoid social situations, exercise classes, dating, or travel because they feel self-conscious or worry about spreading the infection. A rash can sound minor on paper and feel major in real life.
Then there is the household burden. Some patients report family members with similar rashes, which turns one person’s diagnosis into everyone’s laundry problem. Sheets, towels, and clothing suddenly need heat washing. Shared items become suspect. Parents worry about children. Partners worry about skin contact. People start eyeing the couch blanket like it has committed a personal betrayal.
Treatment itself can be stressful. Oral antifungals may work, but they can require weeks of therapy, follow-up visits, medication checks, and careful attention to side effects or drug interactions. Patients may improve slowly rather than dramatically, which can feel discouraging. Even when the fungus is clearing, residual itch or discoloration can make people think the treatment is failing. The recovery is not always emotionally satisfying, even when it is medically successful.
All of that helps explain why doctors are urging earlier recognition. The issue is not only that resistant ringworm is harder to treat. It is that delayed diagnosis turns a manageable infection into a drawn-out, expensive, itchy, and deeply irritating chapter in someone’s life. That is the real story behind the headline.
The Bigger Takeaway
The first confirmed U.S. cases of drug-resistant ringworm matter because they show how even common infections can evolve into more complicated public health problems. Trichophyton indotineae is not the most famous resistant microbe on the block, but it is a reminder that antimicrobial resistance is not confined to hospitals, intensive care units, or dramatic TV plots. Sometimes it arrives as a rash that refuses to leave.
The smart response is not panic. It is awareness. Clinicians need better recognition, better access to testing, and careful antifungal stewardship. Patients need quicker evaluation for severe or stubborn rashes and fewer inappropriate steroid detours. And everyone, frankly, could benefit from remembering that “just a rash” is not always just a rash.
Because when ringworm starts acting like it owns the place, it may be time to call in more than the usual cream.






