Table of Contents >> Show >> Hide
- What Is a Macular Hole?
- Common Symptoms of a Macular Hole
- What Causes a Macular Hole?
- Stages of a Macular Hole
- How Doctors Diagnose a Macular Hole
- Conditions That Can Look Similar
- Treatment Options for a Macular Hole
- What Recovery Is Like After Macular Hole Surgery
- How Successful Is Macular Hole Treatment?
- Possible Risks and Complications
- When to See an Eye Doctor
- Living With a Macular Hole
- Experience-Based Insights: What Patients Often Wish They Knew Earlier
- Conclusion
A macular hole sounds like something your eye made after losing a fight with a tiny hole punch. Thankfully, it is not quite that dramaticbut it is serious. A macular hole is a small opening that develops in the macula, the central part of the retina responsible for sharp, detailed vision. That means reading, driving, recognizing faces, threading a needle, checking your phone, and judging whether your toast is golden or “call the smoke alarm” brown can all become harder.
The tricky part? A macular hole usually does not hurt. It does not wave a red flag. It often begins with blurry or distorted central vision, which many people blame on tired eyes, old glasses, or “just getting older.” But when straight lines start looking bent, letters disappear from the middle of words, or a gray spot shows up in the center of vision, it is time to stop guessing and see an eye care professional.
This guide explains what a macular hole is, how doctors diagnose it, what treatments are available, what recovery may look like, and why early action can make a real difference.
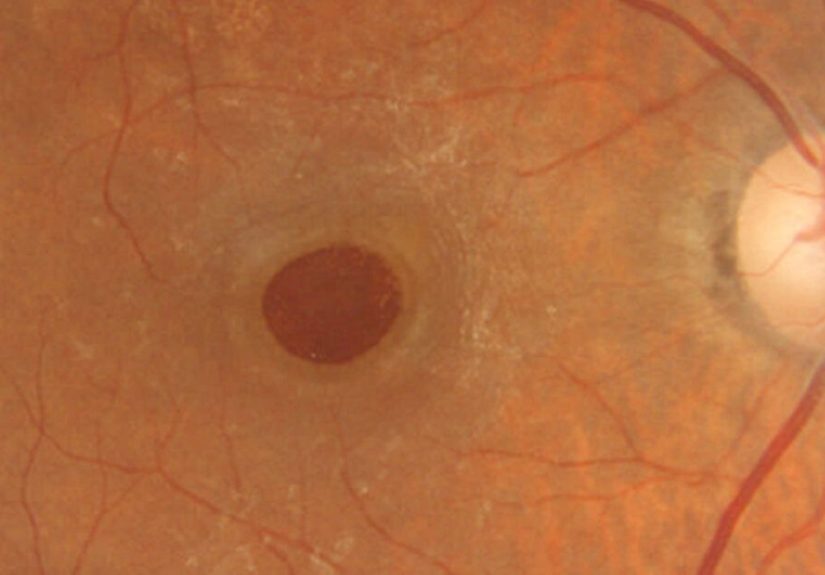
What Is a Macular Hole?
A macular hole is a defect or opening in the macula, the small but mighty area near the center of the retina. The retina lines the back of the eye and works like a living camera sensor, capturing light and sending visual information to the brain. The macula handles fine central visionthe kind used for reading small print, seeing faces clearly, and noticing the difference between a period and a comma. Writers everywhere salute the macula.
Macular holes are usually related to changes in the vitreous, the clear gel that fills the inside of the eye. As people age, the vitreous naturally shrinks and pulls away from the retina. Most of the time, this process happens without major trouble. But sometimes the vitreous tugs on the macula too firmly. That traction can stretch the tissue and lead to a hole.
Macular holes are different from macular degeneration, retinal tears, and diabetic eye disease, although some symptoms may overlap. This is why self-diagnosis is about as reliable as asking your toaster for tax advice. A detailed eye exam is essential.
Common Symptoms of a Macular Hole
The most common symptom of a macular hole is a gradual change in central vision. Peripheral vision usually remains intact, so people may still see movement or objects off to the side. The problem is the center of the visual fieldthe exact spot needed for close detail.
Early Warning Signs
In the early stages, symptoms may be subtle. A person might notice that words look slightly blurred, faces seem less crisp, or straight lines look wavy. Some people describe it as looking through a smudge on a camera lens, except cleaning glasses does not fix it.
Typical macular hole symptoms include:
- Blurred central vision
- Distorted vision, where straight lines appear bent or wavy
- A gray, dark, or missing spot in the center of vision
- Difficulty reading small print
- Trouble recognizing faces
- Reduced sharpness in one eye
- Problems with detailed tasks such as sewing, driving, or using a computer
Because one eye may compensate for the other, symptoms can sneak under the radar. Many people discover the problem only when they cover the stronger eye. That little “cover one eye and look straight ahead” test can reveal distortion that both eyes together were politely hiding.
What Causes a Macular Hole?
Most macular holes are idiopathic, meaning they develop without a clearly identifiable cause beyond age-related changes in the eye. That word sounds fancy, but it basically means, “The eye did this annoying thing on its own.”
Common causes and risk factors include aging, vitreomacular traction, high myopia, eye trauma, inflammation, retinal swelling, and previous retinal conditions. Macular holes are more common in adults over age 60, and they often affect one eye. In some cases, a person may have a higher risk of developing a hole in the other eye, especially if there are similar vitreous changes.
Eye trauma can also cause a macular hole, including blunt injury from sports or accidents. Less commonly, macular holes may be associated with other retinal disorders. The cause matters because it can influence treatment planning and prognosis.
Stages of a Macular Hole
Eye specialists often describe macular holes based on size, depth, and whether the hole is partial-thickness or full-thickness. A partial-thickness defect may affect some layers of the macula, while a full-thickness macular hole extends through the retinal tissue at the center.
Smaller holes and earlier-stage holes generally have better odds of successful closure and stronger visual recovery after treatment. Larger or long-standing holes can still often be treated, but vision improvement may be more limited because the delicate retinal cells have been stretched or damaged for longer.
This is one reason timing matters. Waiting too long because “maybe it will go away after the weekend” can turn a fixable problem into a more stubborn one. Eyes are wonderful, but they do not appreciate procrastination as a medical strategy.
How Doctors Diagnose a Macular Hole
Diagnosing a macular hole usually begins with a careful history and a comprehensive dilated eye exam. The eye doctor will ask about symptoms, when they started, whether one or both eyes are affected, and whether there has been trauma, previous eye surgery, or other eye disease.
Dilated Eye Exam
During a dilated exam, drops widen the pupil so the doctor can examine the retina and macula more clearly. The doctor may use special lenses and a slit lamp microscope to look for changes in the macular tissue. Dilation can make vision blurry and light-sensitive for a few hours, so sunglasses are helpful. Looking mysterious in the parking lot is just a bonus.
Optical Coherence Tomography
Optical coherence tomography, usually called OCT, is one of the most important tests for diagnosing a macular hole. OCT is a noninvasive imaging test that creates detailed cross-sectional pictures of the retina. It allows the doctor to see whether there is a true full-thickness macular hole, a partial-thickness hole, vitreomacular traction, an epiretinal membrane, or another condition that mimics a macular hole.
OCT is especially valuable because it helps measure the size of the hole and guide treatment decisions. It can also track healing after surgery. Think of it as a high-resolution “retina selfie,” but medically useful and much less likely to end up with a weird filter.
Amsler Grid Testing
An Amsler grid may be used to check distortion in central vision. The grid looks like graph paper with a dot in the center. If lines appear wavy, missing, or bent, that may suggest macular involvement. An Amsler grid does not replace a professional exam, but it can help patients monitor changes at home.
Conditions That Can Look Similar
Macular holes can be confused with other retinal conditions. A macular pucker, also called an epiretinal membrane, can cause distortion because a thin layer of scar-like tissue wrinkles the macula. Lamellar macular holes affect part of the retinal thickness rather than creating a full-thickness opening. Age-related macular degeneration can also cause central vision changes, but it is a different disease with different treatment options.
This is where OCT earns its superhero cape. By showing the retinal layers in detail, OCT helps doctors distinguish between these look-alike conditions and recommend the right treatment.
Treatment Options for a Macular Hole
Treatment depends on the type, size, symptoms, and stage of the macular hole. Some early or very small holes may be observed closely, especially if vision is still good and the anatomy suggests a chance of spontaneous improvement. However, many full-thickness macular holes require surgery to close the hole and protect central vision.
Observation for Selected Early Cases
Not every macular hole is rushed straight to the operating room. In selected early cases, a retina specialist may recommend monitoring with repeat OCT scans. The goal is to see whether the traction releases naturally or whether the hole progresses. Patients are usually told to report any worsening distortion, new central blind spot, or sudden drop in vision.
Vitrectomy Surgery
The most common treatment for a full-thickness macular hole is vitrectomy. During this procedure, a retina surgeon removes the vitreous gel that is pulling on the macula. The surgeon may also peel a very thin membrane from the retinal surface, often called the internal limiting membrane, to relieve traction and encourage closure.
At the end of surgery, the surgeon usually places a gas bubble inside the eye. The bubble works like an internal bandage, gently pressing against the macula while the hole seals. Over time, the gas bubble dissolves and is replaced by natural eye fluid.
Vitrectomy is typically performed by a retina specialist, often as an outpatient procedure. The details vary by patient, surgeon, hole size, lens status, and other eye conditions.
Face-Down Positioning After Surgery
Some patients are asked to maintain a face-down position after macular hole surgery. This helps keep the gas bubble pressing against the macula. The required positioning time varies. Some surgeons recommend several days; others use shorter positioning or no face-down positioning in selected cases, depending on surgical technique and the characteristics of the hole.
Face-down positioning can be inconvenient, especially for people with neck, back, breathing, or mobility problems. Patients should talk with their surgeon before surgery about what will be expected. No one wants to learn about face-down recovery for the first time after the procedure, while wearing an eye shield and trying to remember where they left their slippers.
Medication or Drops
Surgery remains the standard treatment for many full-thickness macular holes, but researchers continue to study whether selected small holes may respond to nonsurgical approaches, including topical therapy in specific circumstances. These approaches are not a universal replacement for vitrectomy and should only be considered under the guidance of a retina specialist.
What Recovery Is Like After Macular Hole Surgery
Recovery after macular hole surgery takes time. Vision is usually blurry at first, especially while the gas bubble is still present. Patients may notice a moving line or shadow from the bubble as it gradually shrinks. This can be strange, but it is expected.
The eye may feel scratchy, sore, or sensitive for a short period. Doctors often prescribe eye drops to reduce inflammation and prevent infection. Follow-up appointments are important because the surgeon needs to check eye pressure, healing, and whether the hole is closing.
Important Safety Rules With a Gas Bubble
Patients with a gas bubble in the eye must follow their surgeon’s instructions carefully. Flying in an airplane or traveling to high altitude can be dangerous while a gas bubble remains in the eye because pressure changes can cause the bubble to expand. Certain anesthesia gases must also be avoided until the bubble is gone. Patients should tell every medical professional that they have an eye gas bubble before any procedure.
This is not the moment for “I’ll just wing it.” Eye bubbles and airplanes are not buddies.
How Successful Is Macular Hole Treatment?
Macular hole surgery has a high anatomic success rate, especially for smaller and more recent holes. Many holes close after one operation. Visual improvement is common, but the amount of improvement varies. Some people regain strong reading vision, while others experience partial improvement but still have distortion or reduced sharpness.
Factors that may influence the outcome include the size of the hole, how long it has been present, the patient’s age, the health of the retinal cells, whether there is an epiretinal membrane, and whether other eye conditions such as cataract or macular degeneration are present.
Closing the hole does not always mean vision returns to perfect 20/20 clarity. The retina is delicate tissue, not a cracked phone screen that can simply be replaced at the mall. Still, timely surgery can often prevent further central vision loss and improve daily function.
Possible Risks and Complications
Like any surgery, vitrectomy has risks. Serious complications are uncommon, but they can include infection, bleeding, retinal tear, retinal detachment, increased eye pressure, inflammation, and the need for additional surgery. Cataract formation or progression is common after vitrectomy in people who still have their natural lens.
Patients should contact their surgeon urgently if they experience severe pain, worsening vision, increasing redness, new flashes or floaters, or a curtain-like shadow in vision. These symptoms can signal a complication that needs prompt attention.
When to See an Eye Doctor
Any new distortion, central blur, or missing spot in vision deserves an eye exam. This is especially true if the symptom affects only one eye. A quick self-check can help: cover one eye, look at a door frame, window blinds, spreadsheet, or Amsler grid, and notice whether lines appear straight. Then switch eyes.
Seek care quickly if you notice sudden vision loss, flashes, many new floaters, or a shadow across your vision. Those symptoms may suggest a retinal tear or detachment, which is an urgent condition.
Living With a Macular Hole
Living with a macular hole can be frustrating because the problem affects the exact part of vision people rely on most. Reading may slow down. Screens may need larger text. Night driving may feel more difficult. Recognizing faces from a distance can become awkward, which may lead to accidental “I ignored you at the grocery store” social drama.
Practical adjustments can help. Increase font size on digital devices, use brighter task lighting, reduce glare, try magnification tools, and organize frequently used items in predictable places. People with persistent central vision problems may benefit from low-vision services, even if they still have good peripheral vision.
Experience-Based Insights: What Patients Often Wish They Knew Earlier
Many people who go through macular hole diagnosis and treatment say the hardest part is not the surgery itselfit is the uncertainty beforehand. Vision changes are unsettling, especially when the eye looks normal in the mirror. There is no dramatic swelling, no obvious injury, and usually no pain. That mismatch can make people delay care because they assume the problem is minor.
One common experience is the “one-eye surprise.” A person may be reading, cleaning glasses, or adjusting screen brightness for weeks before realizing the distortion is coming from only one eye. When they finally cover the unaffected eye, the problem becomes obvious. Straight lines bend. Letters vanish. A face on television looks slightly warped. This moment can be alarming, but it is also useful because it pushes the person to schedule an exam.
Another lesson patients often learn is that OCT imaging makes the diagnosis much clearer. Before seeing the scan, “macular hole” may sound abstract and frightening. After seeing the cross-section of the retina, the problem becomes more understandable. The doctor can point to the hole, explain the traction, measure the size, and discuss whether observation or surgery makes sense. A good explanation can turn panic into a plan.
Patients preparing for vitrectomy often benefit from planning the recovery environment before surgery. If face-down positioning is recommended, it helps to arrange pillows, rent or buy positioning equipment if advised, prepare meals, organize eye drops, and set up audiobooks or podcasts. Reading may be difficult during the early recovery period, and the gas bubble can make vision temporarily strange. Entertainment that does not require sharp vision becomes surprisingly valuable. Suddenly, a good podcast is not a luxury; it is a recovery companion with theme music.
People also wish they had asked more questions before surgery. Useful questions include: How large is the hole? How long do you think it has been there? Will I need face-down positioning? How long might the gas bubble last? When can I fly? What symptoms should make me call immediately? Do I have a cataract, and could surgery make it worse? What visual improvement is realistic in my case?
Finally, many patients discover that healing is gradual. The gas bubble shrinks slowly, vision may fluctuate, and the brain needs time to adjust. Some people feel discouraged early on because vision is not instantly crisp. That does not necessarily mean treatment failed. Follow-up OCT scans are often more informative than day-to-day guessing. Patience is not glamorous, but in retina recovery, it is part of the prescription.
Conclusion
A macular hole is a small retinal problem with a big impact on central vision. It can make reading, driving, recognizing faces, and detailed work difficult, often without pain or obvious external signs. The good news is that modern retinal imaging, especially OCT, allows eye specialists to diagnose macular holes accurately and distinguish them from similar conditions.
For many full-thickness macular holes, vitrectomy with membrane peeling and a gas bubble offers a strong chance of closing the hole and improving vision. Outcomes are often better when the hole is smaller and treated earlier. If your central vision becomes blurry, wavy, or missing in one eye, do not wait for your eye to “sleep it off.” Get a professional exam. Your macula may be tiny, but it has a very important joband it deserves a little VIP treatment.
Note: This article is for educational purposes only and is not a substitute for diagnosis, treatment, or personalized advice from an ophthalmologist or retina specialist.





